Article Text

Abstract
Objectives Successful deprescribing depends largely on factors related to the patient. The revised Patients’ Attitudes Towards Deprescribing (rPATD) questionnaire was developed with the objective of evaluating the beliefs and attitudes of older adults and caregivers towards deprescribing. The present study was designed to validate a Spanish version of the rPATD questionnaire, both the versions for older adults and for caregivers, through a qualitative validation phase and the analysis of its psychometric properties.
Design Cross-sectional validation study.
Setting Primary care settings in Málaga (Spain).
Participants A sample of 120 subjects (60 patients with polypharmacy and 60 caregivers of patients with polypharmacy) were enrolled in the study.
Main outcome measures In the qualitative validation stage, the rPATD questionnaire was translated/back-translated and subjected to a cross-cultural adaptation to evaluate its face validity and feasibility. Next, its psychometric properties were assessed. Confirmatory factor analysis was used to evaluate construct validity. Internal consistency was determined using Cronbach’s alpha test. Criterion validity through pre-established hypotheses from the Beliefs about Medicines Questionnaire (BMQ) Specific-Concerns Scale, and test–retest reliability were analysed.
Results Confirmatory factor analysis verified the four-factor structure of the original rPATD questionnaire, with items loading into four factors: involvement, burden, appropriateness and concerns about stopping. The Cronbach’s alpha coefficient of the factors ranged from 0.683 to 0.879. The burden, appropriateness and concerns about stopping factors were significantly correlated with the BMQ Specific-Concerns Score, except for the concerns about stopping factor in the older adults’ version. The consistency of the items between administration times (test–retest reliability) showed weighted Cohen’s kappa values ranging from moderate (>0.4) to very good (>0.8).
Conclusions The Spanish version of the rPATD questionnaire is a feasible, valid and reliable instrument to evaluate attitudes towards deprescribing in Spanish-speaking patients and caregivers.
- Spain
- Polypharmacy
- Deprescribing
- PatientPreferences
- Caregivers
- Psychometric properties
Data availability statement
The raw data underlying the validation process of the Spanish version of the rPATD questionnaire were deposited in Mendeley Data repository (https://doi.org/10.17632/89rz9rgpys.1)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
In this study, we followed the principles of good practices of the International Society for Pharmacoeconomics and Outcomes Research for translation and cultural adaptation of questionnaires.
All data used in this study were self-reported from subjects from primary care setting, which may increase this questionnaire’s external validity.
The sample for the analysis of psychometric properties size was small, which may be considered a limitation, especially when interpreting the results of the confirmatory factor analysis.
The Spanish spoken in Spain was used. The psychometric properties of the questionnaire may vary if it is used in Spanish-speaking subjects from other countries and regions.
Introduction
Polypharmacy is defined as the concomitant use of multiple medicines continuously in the same patient.1 The increase in life expectancy, the intensification of pharmacotherapy and the growing number of patients with multimorbidity have made the prevalence of this phenomenon higher.2 In Spain, its prevalence tripled between 2005 and 2015.3 The negative impact on health includes increased adverse drug reactions, a reduced quality of life, and increased hospitalisations and mortality in older adults.4–6
Deprescribing is the process of withdrawal of an inappropriate medication, supervised by a healthcare professional, with the goal of managing polypharmacy and improving outcomes.7 It is a safe process that provides benefits in terms of quality of life and cost reduction for patients and health systems.8 9
Successful deprescribing will depend on factors related to the health and social system itself, the physician, the patient and the relationship between all of them.10 11 Every day, there is more evidence on the importance of involving patients in decision-making concerning deprescribing.12–14 This is accompanied by a fundamental ethical argument: respecting patient autonomy requires a detailed discussion of the benefits and risks of taking medications.15
However, in clinical practice, shared decision-making is influenced by multiple factors, and there is wide variability depending on the situation and between different physicians. Physicians may be reluctant to initiate conversations about deprescribing because they falsely perceive their patients as having a medication dependence or out of fear that the patient could interpret the deprescribing attempt as their care being abandoned.16 17 Among the patient-dependent factors are the degree to which they trust medical advice, any cognitive biases leading them to only listen to positive information, difficulties in processing information and the lack of tools that allow them to explore their preconceived notions regarding deprescribing.18 19
With the objective of exploring the beliefs that patients have about the number of medications they are taking and under what circumstances they would be willing to start a deprescribing process, Reeve et al developed the Patients’ Attitudes Towards Deprescribing (PATD) questionnaire20 and later its revised version (rPATD), which has a version for older adults and another for caregivers.21 There is also a version of the rPATD questionnaire adapted for people with mild cognitive impairment and mild-to-moderate dementia (rPATDcog).22 The rPATD questionnaire constitutes a further step in the so-called deprescribing rainbow: a conceptual framework in the form of concentric arcs, with five determinants of deprescribing: the clinical, psychological, social, economic and physical planes, with the patient himself in the centre of the arc.23 This revised version expands the view to the entire spectrum of the theoretical construct and analyses four factors: the level of involvement and knowledge of the medications (involvement factor), the drawbacks related to the medications (burden factor), the belief in the need for medications and possible secondary effects (appropriateness factor) and the possibility of medication stoppage and the feelings that this would generate (concerns about stopping factor).
The rPATD questionnaire was originally developed in English. It has been translated into other languages, including Dutch,24 Amharic25 and Malay,26 although it has only been formally validated into Arabic,27 Danish28 and French.29 To date, it has not been validated into Spanish.
Aim of the study
To validate a Spanish version of the rPATD questionnaire, both the versions for older adults and for caregivers, through a qualitative validation phase and the analysis of its psychometric properties.
Materials and methods
The questionnaire consists of 22 and 19 items, respectively, in the versions for older adults and caregivers. It covers the four factors studied as well as two global questions. An investigation based on two stages was designed: a first qualitative validation and a second analysis of the psychometric properties of the questionnaire to analyse its validity (construct validity and criterion validity) and reliability (internal consistency and test–retest reliability) (figure 1). Authorisation was obtained from the authors of the questionnaire to undertake this study. The study was conducted between February 2019 and January 2020.

Flow chart of the progress through the qualitative validation phase and analysis of the psychometric properties. rPATD, revised Patients’ Attitudes Towards Deprescribing.
Qualitative validation
The objective of this stage was to evaluate the face validity and feasibility of the Spanish questionnaire. It was developed using a method structured in five steps following the principles of good practices of the International Society for Pharmacoeconomics and Outcomes Research Task Force for Translation and Cultural Adaptation30:
Direct translation of the questionnaire from English to Spanish by two professional bilingual translators.
Analysis of the discrepancies between the two translations by the research team to obtain a synthesis version.
Back-translation of the Spanish synthesis version into English by two different professional translators. Items without complete equivalence with the original version were indicated.
Consolidation: the synthesis version was evaluated by a multidisciplinary group of 10 experts: a linguist, a specialist in family medicine, one in internal medicine, two in clinical pharmacology, one expert in public health, two primary care pharmacists, one hospital pharmacist and one nurse. Each expert evaluated from 1 to 10 the degree of comprehensibility of each item and the equivalence of the item of the synthesis version to the original version. For those items whose mean was <7.50 points for comprehensibility or equivalence, alternative wording was proposed. They were also asked to add comments to each item if necessary.
Pilot with a group of nine patients and seven caregivers selected by consecutive sampling to evaluate their reactions when filling in the questionnaire, detect possible errors, analyse the comprehension of the items and assess the alternative wordings proposed. The selection criteria were the same as in the subsequent phase of analysis of the psychometric properties of the questionnaire (see Setting and sampling). These subjects were different from those who participated in the next phase.
At this point, the first Spanish version of the questionnaire was obtained.
Psychometric properties
Setting and sampling
An observational cross-sectional validation study was designed. Subjects aged 18 years and older who were taking five or more medications (duration ≥6 months) were selected by consecutive sampling from three urban primary care health centres in Málaga (Spain). Sampled were the consecutive patients or caregivers who attended a scheduled family medicine consultation stratified according to each of the three participating centres of the study.
The sample for patients was made of subjects capable of completing the questionnaire by themselves. In the event that the subject could not complete the questionnaire due to physical and/or intellectual disability, determined by the doctor who cared for him in the family medicine consult, the main caregiver was asked to complete the caregivers’ version, thus establishing the sample for caregivers. Subjects with a physical and/or intellectual disability preventing them from completing the questionnaire and who did not have a primary caregiver were excluded. All subjects who met the selection criteria were selected from the day established as the start of data collection until the sample size was completed.
There is no consensus on calculating sample size for translation studies or questionnaire validation. Recommendations for the sample size in factor analysis range from 3 to 10 subjects per variable (item)31 with a minimum of 50.32 Bujang et al support the ratio 3 subjects per variable when the response scale has at least 4 levels.33 Given that the rPATD questionnaire has 22 and 19 items in its two versions, a total sample size of 120 subjects (60 patients and 60 caregivers) was set. Questionnaires with more than 2 blank items would be excluded.
Study variables
Sociodemographic and clinical variables (comorbidities and number of regular medications) were collected through a researcher-administered form developed for this study. The patient or caregiver was asked to bring all the medication to the interview in order to check the number of regular medications. We also collected the responses to the self-completed rPATD questionnaire and to the Spanish version of the Beliefs about Medicines Questionnaire (BMQ) Specific-Concerns Scale.34 The characteristics of the subjects were analysed using descriptive statistical measures.
Construct validity: confirmatory factor analysis
Confirmatory factor analysis (CFA) was used to determine whether the obtained data fitted into the assumed structure of the rPATD questionnaire. Before running CFA, the presence of outliers and the multivariate normality were evaluated. The first step, based on theoretical considerations, was the estimation of a correlated four-factor CFA without allowing cross-loadings, and fixing to one the variance of the factors as well as the loading of the first item of each factor. Once the initial model was estimated, we proceeded to evaluate model fit, modification indices and model parameters, in order to improve this initial model. Additionally, we compared the initial model with a one-factor solution and an uncorrelated four-factor solution, through Likelihood Ratio Tests.
The goodness of fit was evaluated through Root Mean Square Error of Approximation (RMSEA) and the 90% CI as well as a test of close fit (p of close fit) (It takes values ranging from 0 to 1. Good fit: RMSEA ≤0.05, acceptable fit: 0.05 ≤RMSEA ≤ 0.08, and poor fit: RMSEA ≥0.1), Standardised Root Mean Square Residual (Its values range from 0 to 1. It is considered a good fit when SRMR ≤0.08), Normed Fit Index (Very good fit: NFI ≥0.95, marginal/acceptable fit: 0.90 ≤ NFI < 0.95, and poor fit: NFI <0.90), Comparative Fit Index (Very good fit: CFI ≥0.95, marginal/acceptable fit: 0.90 ≤ CFI < 0.95, and poor fit: CFI <0.90) and Incremental Fit Index (Values ≥0.90 are considered good). The choice of the selected indices and their thresholds for determining a good fit were established following Kline.35
Convergent validity of the model was evaluated through squared root of McDonald’s omega coefficient of each factor (the better the closer to one).36 Discriminant validity was evaluated by Heterotrait-Monotrait ratio of correlation (HTMT) (values higher than 0.85 indicate discrimination problems).37 38
As expected with ordinal scales, multivariate normality testing rejected the hypothesis of multivariate normality for both versions of the questionnaire. Therefore, maximum likelihood estimation with robust standard errors was used for estimating the models, since this estimator is not affected by this absence of multivariate normality.
Internal consistency
The internal consistency of each of the factors of the questionnaire was determined using Cronbach’s alpha test. This coefficient analyses the correlation of the items considering how each of the different items measures the same characteristics. It ranges from 0 to 1 and its interpretation is similar to a correlation coefficient: the more the homogeneity, the closer the value 1. Cronbach’s alpha values of 0.7 or higher indicate acceptable internal consistency.39
Criterion validity
Three factors (burden, appropriateness and concerns about stopping) were interpreted by the authors of the original questionnaire to potentially predict a willingness to have a medication deprescribed.21 As in the validation of the original questionnaire, it was hypothesised that these three factors would be related to the BMQ Specific-Concerns Score (burden score and concerns about stopping score directly and appropriateness score inversely), meaning there would be a statistically significant gamma rank correlation coefficient.
Test–retest reliability
A second interview was conducted 2–3 weeks later to administer the questionnaire again to a subgroup of 20 patients and 20 caregivers extracted by simple random sampling of the total sample. The gamma rank coefficient for each factor and the weighted Cohen’s kappa coefficient (linear) were calculated for each individual item. The weighted Cohen’s kappa coefficient was considered poor (<0.20), fair (0.20–0.40), moderate (0.41–0.60), good (0.61–0.80) or very good (>0.80).40
Score and time to complete the questionnaire
Each question was scored on a Likert scale with five response options to obtain a general score for each item and for each factor. Similar to the original questionnaire, greater agreement with the items of the factors involvement, burden and concerns about stopping would correspond to higher values on the scale (5: strongly agree; 4: agree; 3: unsure; 2: disagree; 1: strongly disagree), while the items of the appropriateness factor were scored inversely since a greater acceptance of the items of this factor implied a lower perception of having an appropriate medication.
The time taken to complete the questionnaire was recorded for each participant.
Patient and public involvement
Neither patients nor public were involved in the design or planning of this study.
Statistical packages
The statistical calculations were performed with the IBM Statistical Package for Social Sciences Statistics V.22.0 for Windows. CFA was performed using R Statistical Software, packages lavaan,41 semTools,42 psych43 and MVN.44 The level of statistical significance was established at a value of p<0.05.
All data generated in this study were deposited in Mendeley Data repository.45
Results
Qualitative validation
Face validity was verified through the qualitative validation process. After the translation/back translation, in the consolidation phase only one item (G2, caregivers’ version) had a score ≤7.5 points for comprehensibility, so an alternative phrasing was proposed. Modifications were also made to certain items following the comments of the group of experts. In the pilot study, the questionnaire was administered to nine patients (mean age 68.8 years, range 51–83) and seven caregivers (mean age 54.6 years, range 45–72). This was continued until saturation of the information extracted from the interviews. At the end of this phase, the research team considered the questionnaire feasible for its application.
Psychometric properties
Characteristics of the sample and analysis of the responses
77 patients and 72 caregivers were offered to participate in the study, of whom 60 patients and 60 caregivers completed the questionnaire (response rates of 77.9% and 83.3%, respectively). Those who refused to participate cited lack of time (67.9%), reluctance to participate in a research study (7.1%) or other unspecified reasons (25%). The characteristics of the participants are shown in table 1. No questionnaire presented more than two blank items, so none was excluded. The descriptive analysis of the responses to both versions of the questionnaire is detailed in online supplemental appendix 1.
Supplemental material
Participant characteristics (older adults n=60, caregivers n=60)
Construct validity: CFA
In the correlated four-factor model of the version for older adults, we found a non-significant loading of B1, and loading values <0.5 of I4, A5, C2 and C4. We also found a low correlation of the involvement factor with the burden and concerns about stopping factors. Modification indices indicated a possible improvement if the correlation between B3 and B5 was allowed. Based on these findings, we finally selected a model with the following specifications: the loading of B1 was set to 0, the loadings (not standardised) of the items I4, A5, C2 and C4 were set to the same value, the correlation between B3 and B5 was allowed and the correlation of the involvement factor and the burden and concerns about stopping factors was set to 0.
The model had 44 free parameters and 169 degrees of freedom. The global fit of the model based on the χ2 test (χ2 (169)=177.518, p=0.311) indicated that the proposed model fitted the data. Both the Akaike Information Criterion (AIC) and the Bayesian Information Criterion (BIC) of this model were lower than those of the initial model (AIC: 2886 vs 2910, BIC: 2967 vs 2996). The fit indices showed an acceptable-good fit. RMSEA showed a good fit, with a 90% CI 0.000 to 0.070, and a p value of 0.743 (table 2).
Model fit indices for older adults’ and caregivers’ versions
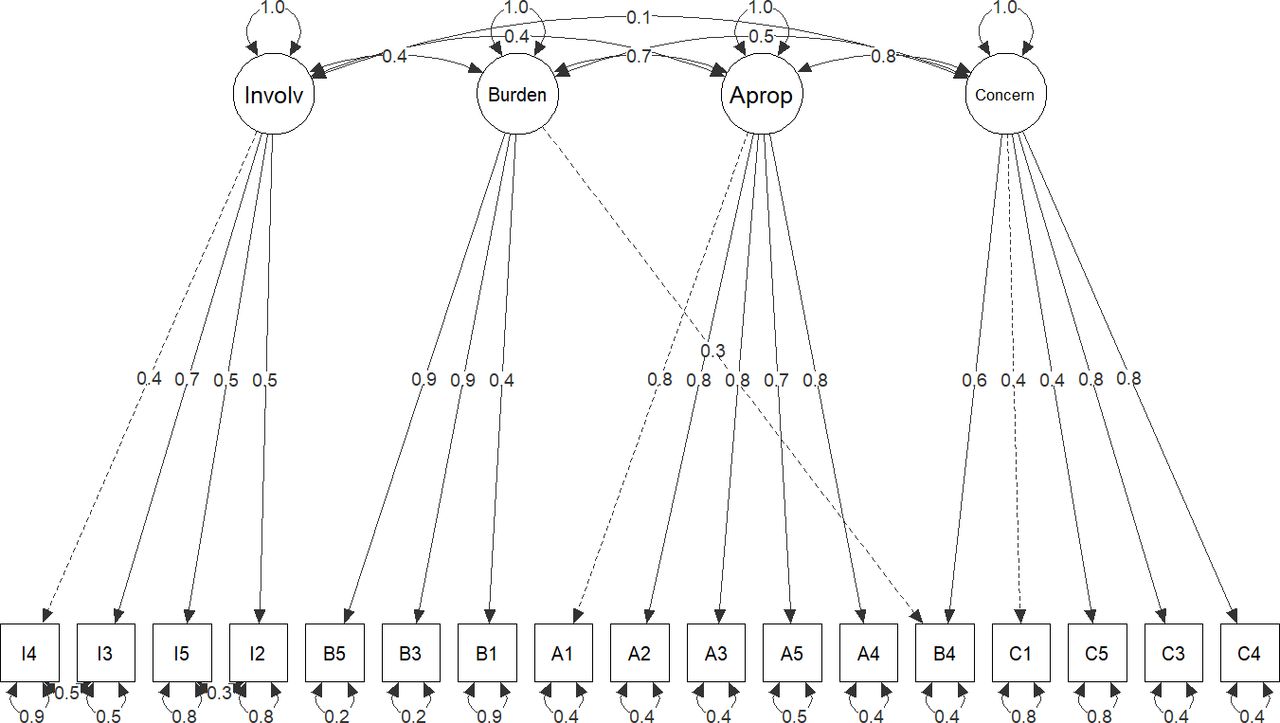
All standardised loadings were statistically significant, ranging from 0.45 to 0.86 (see online supplemental appendix 2). In the selected model, the correlations were statistically significant among all the factors except between burden and concerns about stopping factors. The factor structure model of the older adults’ version of the questionnaire is presented in figure 2.
Supplemental material

Factor structure model and estimated value of the standardised loadings of the older adults’s version of the revised Patients’ Attitudes Towards Deprescribing questionnaire. The dashed lines indicate the first item of each factor, whose loading was set to 1 in the initial model. Involv, Involvement factor; Burden, Burden factor; Approp, Appropriateness factor; Concern, Concerns about stopping factor.
No modification index was higher than 10. The matrix with the differences between the empirical and the implicit variance–covariance matrices can be consulted in online supplemental appendix 3. Both the convergent validity and discriminant validity of the model were adequate. McDonald’s omega showed values of 0.797, 0.803, 0.802 and 0.722 for the involvement, burden, appropriateness and concerns about stopping factors, respectively. The matrix with the discriminant validity associated to the four factors based on the HTMT criterion is presented in online supplemental appendix 4.
Supplemental material
Supplemental material
In the initial correlated four-factor model of the version for caregivers, we found a non-significant loading of I5 and I2, and loading values <0.5 of B1 and C5. Modification indices indicated a possible improvement if the correlation between I4 and I3, and between I5 and I2 was allowed, as well as the loading of B4 in the concerns about stopping factor. Based on these findings, we selected a model with the following specifications: the non-standardised loadings of the variables I5, I2, B1 and C5 were set to the same value, and the correlation between I4 and I3, and between I5 and I2 was allowed. Besides, the loading of B4 in the concerns about stopping factor was allowed, and its loading was set to 1 in its factor of origin (burden factor).
The model had 43 free parameters and 113 degrees of freedom. The global fit of the model based on the χ2 test (χ2 (136)=119.32, p=0.324) indicated that the proposed model fitted the data. Both the AIC and the BIC of the model were lower than those of the initial model (AIC: 2729 vs 2764, BIC: 2686 vs 2719). The fit indices revealed an acceptable-good fit. RMSEA showed a good fit, with a 90% CI 0.000 to 0.075), and a p value of 0.713 (table 2).
As in the older adults’ version, all standardised loadings were statistically significant, ranging from 0.35 to 0.89 (see online supplemental appendix 2). The only significant correlations observed in the selected model were between the appropriateness factor and the concerns about stopping and burden factors. The correlations of the involvement factor with the rest of the factors were higher than in the older adults’ version, although they remained low. The factor structure model of the caregivers’ version of the questionnaire is presented in figure 3.

{kind=link}
{kind=link}
{kind=link}
Factor structure model and estimated value of the standardised loadings of the caregivers’ version of the questionnaire. The dashed lines indicate the first item of each factor, whose loading was set to 1 in the initial model. Involv, Involvement factor; Burden, Burden factor; Approp, Appropriateness factor; Concern, Concerns about stopping factor.
No modifying index exceeded the value of 10. The matrix with the differences between the empirical and the implicit variance–covariance matrices is presented in online supplemental appendix 3. Convergent validity of the model was adequate for the burden, appropriateness and concerns about stopping factors (McDonald’s omega values of 0.639, 0.881 and 0.694, respectively), although it was poor for the involvement factor (0.482). Discriminant validity based on the HTMT criterion was adequate, except for the appropriateness factor (see online supplemental appendix 4).
Internal consistency
The Cronbach’s alpha values for the factors of the questionnaire were exemplary (>0.8) or extensive (>0.7). The concerns about stopping factor of the caregivers’ version showed a Cronbach’s alpha score of 0.683, which was considered moderate39 (table 3).
Results of internal consistency and test–retest reliability of the Spanish version of the revised Patients' Attitudes Towards Describing questionnaire
Criterion validity
The three factors (burden, appropriateness and concerns about stopping) were statistically significantly correlated with the BMQ Specific-Concerns Score, except for the concerns about stopping factor in the older adults’ version (p=0.189). Higher burden and concerns about stopping scores were directly correlated with a higher BMQ Specific-Concerns Score, while the appropriateness score was negatively correlated, as it was hypothesised (table 4).
Results of the criterion validity analysis
Test–retest reliability
The subgroup of patients and caregivers to whom the questionnaire was readministered had a mean age of 64.3 and 56.6 years (IQR 58.0–72.7 and 46.0–67.0, respectively). The correlations are shown in table 3.
Time to complete the questionnaire
The average time it took to fill in the questionnaire was 5:21 min (SD 2:43) for the older adults’ version and 4:36 min (SD 1:04) for caregivers’ version. It took the majority of participants <5 min to complete the questionnaire (61.6% and 67.4%, respectively) and most of the others 5–10 min (33.3% and 28.3%, respectively).
Discussion
Summary of findings
The objective of this study was to validate the rPATD questionnaire into Spanish for both patients and caregivers. Several questionnaires analyse the knowledge, attitudes and relationship of patients towards their medications46–49 and their perceptions of deprescribing.50 The former focus on analysing patients’ beliefs about their medications, adherence and the medication-related burden. The latter examine the motivation behind deprescribing and the patients’ relationship with the medication provider. The rPATD questionnaire combines these elements into four factors and two global items of clinical relevance.
An exhaustive qualitative validation process was performed. After this stage, the Spanish version of the rPATD questionnaire showed adequate face validity and feasibility.
The CFA presented in this study confirmed the four-factor structure of the rPATD questionnaire. Certain items showed low loadings in their respective factors. In both versions, a low loading of B1 (money/expensive medicines) in the burden factor was found. This could be explained because participants with different levels of contribution for the payment of medications were selected for the study. In Spain, this contribution ranges from 0% to 60% depending on income, type of medication and employment situation, which can make them perceive medication spending as a burden or not.51 This item was retained in the burden factor due to its perceived importance and its utility in evaluating how a possible change of contribution would affect the patient or caregiver.
In the older adults’ version, the correlation established between B3 (large number of medicines) and B5 (too many medicines) is logical. The difference between both items is very subtle and only focusses on the nuance of the expression ‘too many’, which indicates that, regardless of whether the patient is taking a large number of medications or not, he thinks that he should take fewer medications than those he is taking.
In the caregivers’ version, item B4 (burden) loaded on more than one factor (burden and concerns about stopping factors). This has external validity, since, as will be discussed later, caregivers concerned about the burden of the medication may also show high levels of concern about its cessation, reflecting high levels of concern in general. In the exploratory factor analysis of the original rPATD, three items of the older adults’ version and one of the caregivers’ version loaded on more than one factor.21 However, this limitation is considered irrelevant in practice. Also in the caregivers’ version, the correlation was allowed between items I4 (involved in decisions) and I3 (know as much as possible), and between I5 (always ask if I don't understand) and I2 (know current medicines). These are closely related items, although being located contiguously in the questionnaire, a response bias can not be discarded. This kind of bias reflects the tendency of the individual to respond in the same way as the previous item, particularly when response options consist of Likert scales keyed in the same direction.52
In general, in both versions the involvement factor showed a low correlation with the other factors. This is not surprising as, while the other three factors (burden, appropriateness and concerns about stopping) were identified as possible predictors of deprescribing in the original validation of the questionnaire, the involvement factor was included as a provider of additional relevant information for clinical practice.21 The findings observed in this CFA are consistent with this approach.
The internal consistency of the factors of the questionnaire showed Cronbach’s alpha values that mostly exceeded the commonly established cut-off of 0.7. These values are similar to those of the validated original questionnaire. Cronbach’s alpha, as a measure of the correlation of the items comprising a scale, is an inherent property of the response pattern of a specific sample and not a characteristic of the scale itself. Hence, this measure is important when validating a measurement instrument in a sample with different characteristics from the original sample.
The BMQ Specific-Concerns Scale analyses the patients’ concerns about their medications related to taking medication, long-term effects, knowledge of medication, and interference in their daily life, and possible dependence. Therefore, it would be expected that a greater perceived concern about the medication would correspond to a greater perceived burden, and conversely, with a lower concern about stopping medication and a worse perception of appropriate use. However, in the validation of the original questionnaire, contradictory to what would be expected, a greater perceived concern about the medication as measured by the BMQ Specific-Concerns Scale was correlated with a greater concern about stopping the medication. This may represent more than an underlying fear about stopping medications but may also be a reflection of people who experience high levels of stress or worry in general. In the present study, we hypothesised that we would see the same results as observed in the validated original questionnaire. The expected correlations were found in both the adult and caregiver samples. Only the correlation with the concerns about stopping factor of the older adults’ version was not statistically significant. This is consistent with what was explained above.
The Spanish version of the rPATD questionnaire was show to be reliable. The results of the weighted Cohen’s kappa coefficient of the items showed moderate to very good values, slightly higher than those of the original rPATD questionnaire. The reproducibility of the factors was also higher than that on the original questionnaire. These slight differences between both studies may be due to the characteristics of the sample used, since in the present study patients with polypharmacy were selected, who may have stronger opinions and, because of their greater history of medication, may be more prone to remember the answers, producing a memory bias. The time elapsed between administration and readministration of questionnaires was similar in both studies.
A common concern in the use of questionnaires is the time it takes to complete them. Longer questionnaires have a lower response rate, which can limit their usefulness.53 We analysed the time spent completing the questionnaire, which was similar to the time spent in the original one, where 62.1% of older adults and 50% of caregivers completed the questionnaire in <5 min. These results make its use viable in daily clinical practice as well as in research.
Strengths and limitations
The original rPATD questionnaire was validated in patients taking one or more medications. In this study, patients with polypharmacy were defined as those taking at least five medications, since this is the most accepted definition in the medical literature and has a greater predictive value for medication-related adverse effects.54 Using an in-person questionnaire exclusively in subjects from the primary care setting was prioritised over both in-person and online administration of the original validation study, which may have increased this questionnaire’s external validity. In the same way, although the target population in the original validation study was older adults (>65 years of age), we did not establish any age limit, similarly to the validation of the Arabic version of the questionnaire,27 in order to generalise its use to patients with polypharmacy and not only older adults. Despite this, the four-factor structure of the original rPATD questionnaire was maintained.
The fit indices found in the CFA, in general, showed an acceptable-good fit for both versions of the questionnaire, although optimal results were not achieved for all of them. This could be related to the relatively small sample size of the study, which could be considered a limitation to take into consideration when interpreting the results of the CFA. In addition to this, although we have followed the thresholds established by Kline, different simulation studies have shown that these thresholds can vary depending on both the sample size and the distribution of the variables.55
In the test–retest reliability analysis, while the research team considered using the intraclass correlation coefficient instead of the weighted Cohen’s kappa coefficient since the latter has several limitations, such as its dependence on the prevalence of responses in each category and the number of categories,56 using the same coefficients as the original questionnaire was prioritised, to compare results.
This questionnaire investigates beliefs and attitudes towards deprescribing, but whether the patient will want to be deprescribed in real life remains to be seen. Although qualitative studies have hinted in this direction,57 58 the tools analysed so far, such as the PATD questionnaire and the BMQ questionnaire, have demonstrated a low predictive value for a successful deprescribing.59
Future use in research and clinical practice
In the validation of the questionnaire, the Spanish spoken in Spain was used. The Spanish version of the rPATD questionnaire allows its use in research on Spanish-speaking people as well as comparisons among population groups, although it is true that Spanish varies regionally and that the cultural characteristics and health systems are different. A future challenge is to analyse the psychometric properties of the questionnaire in these regions.
The adaptation of a Spanish version of the rPATDcog questionnaire and its administration to patients with cognitive impairment is another challenge for future research.
Engaging patients, family and caregivers and focussing on their perspectives have been identified as a priority in deprescribing research.60 The rPATD questionnaire has been used to analyse attitudes of patients and caregivers towards deprescribing in general61–63 and in specific pharmacological groups.24 Regarding its use in clinical practice, identifying those patients with a favourable predisposition to deprescribing can be useful to initiate the negotiation of a medication withdrawal process. In addition, obtaining a score for each factor provides information on the different aspects of deprescribing and can serve as a guide to the needs of patients in this process. The rPATD questionnaire, administered alone or integrated within other, more complex interventions, can improve the adequacy, adherence and reconciliation of medication of the patient with polypharmacy.
Conclusions
The Spanish version of the rPATD questionnaire for patients and caregivers showed psychometric properties that demonstrated adequate feasibility, validity and reliability for use in both clinical practice and research in Spanish-speaking people. The future challenges are to analyse the predictive value of the Spanish version of the rPATD questionnaire for deprescribing as well as how well the questionnaire performs when applied to Spanish-speaking individuals from regions other than that of the present study.
A copy of the Spanish version of the rPATD questionnaire is available in online supplemental appendix 5.
Supplemental material
Data availability statement
The raw data underlying the validation process of the Spanish version of the rPATD questionnaire were deposited in Mendeley Data repository (https://doi.org/10.17632/89rz9rgpys.1)
Ethics statements
Patient consent for publication
Ethics approval
Approval for both phases of the study (qualitative validation and psychometric properties) was granted by the Research Ethics Committee of Málaga, Spain (ID: 0611-N-17). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors wish to thank Emily Reeve and Francisca Leiva for their advice throughout the design and execution of the project, and Francisco Javier Barón for his valuable suggestions during data analysis and its interpretation. They also wish to thank the workers of the Palma-Palmilla, Alameda-Perchel, and Victoria health centres (Málaga, Spain) for their invaluable help.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @joseignaciojr
Contributors JIdJ-R, AJG-R and EG-M designed the study and performed statistical analysis and contributed to interpretation of findings. JIdJ-R, MC-J, AG-H and CS-S collected the data. JIdJ-R and EG-M drafted the initial manuscript. All authors contributed substantially to its revision. JIdJ-R is responsible for the overall content as guarantor.
Funding This investigation was supported by the “Isabel Fernández Scholarship to support doctoral theses” of the Spanish Society of Family and Community Medicine (SEMFYC) (2017 call) and the “Isabel Fernández Scholarship to support doctoral theses” of the Andalusian Society of Family and Community Medicine (SAMFYC) (2017 call).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.