Article Text

Abstract
Purpose The Taicang and Wuqiang cohort study (TAWS) was established to examine the association between early-life nutrition and children’s health, and to explore the potential roles of maternal health, metabolites and microbiota in children’s health in two different regions of China.
Participants A total of 7041 mother–child pairs were recruited during early pregnancy (n=4035, 57.3%) or delivery phase (n=3006, 42.7%) from health centres or hospitals in Taicang and Wuqiang. Mother–child pairs were followed up three times during pregnancy, once during delivery, and 7–10 times in the 3 years after delivery. Questionnaires were used to collect data on diet, supplementary intake, physical activity, depression scale, disease occurrence, feeding practice and development quotient of children. Anthropometric measurements of mothers and their children were assessed at each visit. Pregnancy outcomes were extracted from medical records. Biospecimens were collected and stored, including venous blood, cord blood, urine, stool, breast milk, cord and placenta.
Findings to date Data from the TAWS cohort showed different baseline characteristics of participants at the two sites of TAWS. Abnormal metabolism occurred among newborns whose mothers were diagnosed with gestational diabetes mellitus. Maternal serum folic acid above 14.5 ng/mL at early pregnancy was associated with a reduced risk of delivering small-for-gestational-age newborns.
Future plans The association between maternal nutrition and the health of offspring will be examined at various follow-up visits. Biomarkers will be analysed to assess the associations between early-life nutrition and child development, immunity and health. Strategic recommendations for optimal infant feeding practices, obesity prevention and routine healthcare items will be developed and proposed based on the findings from the study. Children in this prospective cohort study will be followed up once a year until age 12 years to further examine the relationships between early-life nutrition and children’s long-term development and health.
- cohort study
- early-life
- nutrition
- mother
- child
Data availability statement
Data are available upon reasonable request. Data are available on reasonable request, including anthropometric data and micronutrient status data of mothers and children.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This ongoing study collected data from three follow-ups during pregnancy, one follow-up during the delivery phase, and 7–10 follow-ups after birth; it provides rich data with respect to dietary information and biospecimens to explore the mechanisms of associations between maternal and early-life nutrition and children’s growth and health.
The Taicang and Wuqiang mother–child cohort in China included two study sites, one in a wealthy southern city and the other in a poor northern county; findings from this cohort may improve the understanding of diverse maternal diets and lifestyle patterns in China.
Study participants may not be representative of the overall relevant population, as ineligibility or unwillingness information was not well documented; additionally, some participants were lost to follow-up, and biological samples were obtained from only a subset of participants, which may have led to some selection bias.
Introduction
Evidence from epidemiological studies and animal models has bolstered the paradigm of ‘developmental origins of health and disease’ over the past decades.1–4 It is now well established that the first 1000 days of life (ie, from conception to the age of 2 years) is a critical time window for developmental trajectory programming.5 6 Adverse disturbances that occurred during this period may lead to increased risks of chronic diseases across one’s lifespan or an epigenetic transgenerational inheritance of such risks.7–10 Of particular importance, extensive evidence suggests that maternal diets and early-life nutritional status are associated with altered risks of both short-term and long-term diseases for the offspring, including metabolic, immunological, mental and reproductive diseases.10–13 Consequently, achieving optimal nutrition during pregnancy and early life can be one critical step to substantially lower the future disease burdens.
China has the largest population worldwide, with around 15 million babies born each year.14 15 Given the population size, addressing early-life nutrition to prevent future diseases has tremendous benefits in lowering the social and economic burdens associated with these negative long-term consequences. Since the 1990s, China has made significant improvements in maternal and child health, meeting the Millennium Development Goals and Sustainable Development Goals.16 17 In parallel with rapid economic growth and improved healthcare coverage, China is on the way of further closing the gaps in maternal and newborn care across regions.18 19 Of note, studies have suggested heterogeneity in maternal and infant health profiles across different geographical regions in China: rates of obesity-related maternal or infant complications are higher in more developed settings, whereas rates of undernutrition-related complications are more common in less-developed settings, possibly due to differences in socioeconomic status, access to food choices, dietary patterns or a combination of these factors.18–21
To date, a few birth cohorts in China have examined the associations between several environmental pollutants, nutrients (eg, folic acid and vitamin D), nutrition in pregnancy, maternal biomarkers and birth defects or children’s health.22–25 Although biospecimens were collected in some of these established cohorts, only routine subclinical indicators related to nutrition were assessed and examined. In addition, few Chinese cohort studies have collected up-to-date data reflecting the recent economic development and dietary intake with child growth or health. Furthermore, studies representing different Chinese subgroups are needed to account for the noted differences in maternal and infant health profiles when examining maternal and early-life nutrition. To fill in these critical gaps, we sought to establish a multicentre cohort, aiming to improve our understanding of the role of early nutrition on children’s development (anthropometric and psychological development) and health (nutritional status, the occurrence of anaemia, fever, diarrhoea, allergy, etc); and to explore potential mechanisms (metabolomics, microecology, immunology) and promote general healthcare across different regions of China.
Cohort description
Cohort set-up and quality control
The Taicang and Wuqiang Study (TAWS) consisted of two study sites: Taicang (Jiangsu Province, China) and Wuqiang (Hebei Province, China). It was designed and supervised by the National Institute for Nutrition and Health (NINH), formerly named National Institute for Nutrition and Food Safety. Study participants were screened, recruited, and followed separately at local healthcare centres and obstetric hospitals of the two study sites.
The Taicang subcohort was hosted by the Taicang Service Center for Mother and Child Health and Family Planning. Among 22 community health centres, doctors at the prenatal clinics and child care clinics took charge of the recruitment and the follow-up during pregnancy and post partum. Nurses at the obstetric clinics of all five hospitals were responsible for the follow-up during the delivery phase. The Wuqiang subcohort was hosted by the Wuqiang Center for Disease Control and Prevention. Doctors in all eight township health centres and the Maternal and Child Health Hospital were responsible for the recruitment and the follow-up during pregnancy and post partum, and nurses at the obstetric clinic of Wuqiang County Hospital took charge of recruitment and follow-up during the delivery phase.
One month before recruitment, all the doctors and nurses involved in the study at the two study sites received 16 hours of training. Training contents included participant recruitment, questionnaire information collection (basic characteristics, supplementary intake, physical activity, depression scale, disease occurrence or medication), dietary measurements (3-day food records; Food Frequency Questionnaire (FFQ)), anthropometric measurements and assessments, child feeding, development quotient (DQ) test, biological sample collection and preservation, follow-up appointment and data entry. Since the initiation of recruitment, training sessions were held every 2 months for the first 2 years and quarterly thereafter. Training contents during the study were designed to address the problems identified in the supervision of the principal investigators and questions raised by study doctors and/or nurses, and each training session lasted 1 hour or longer.
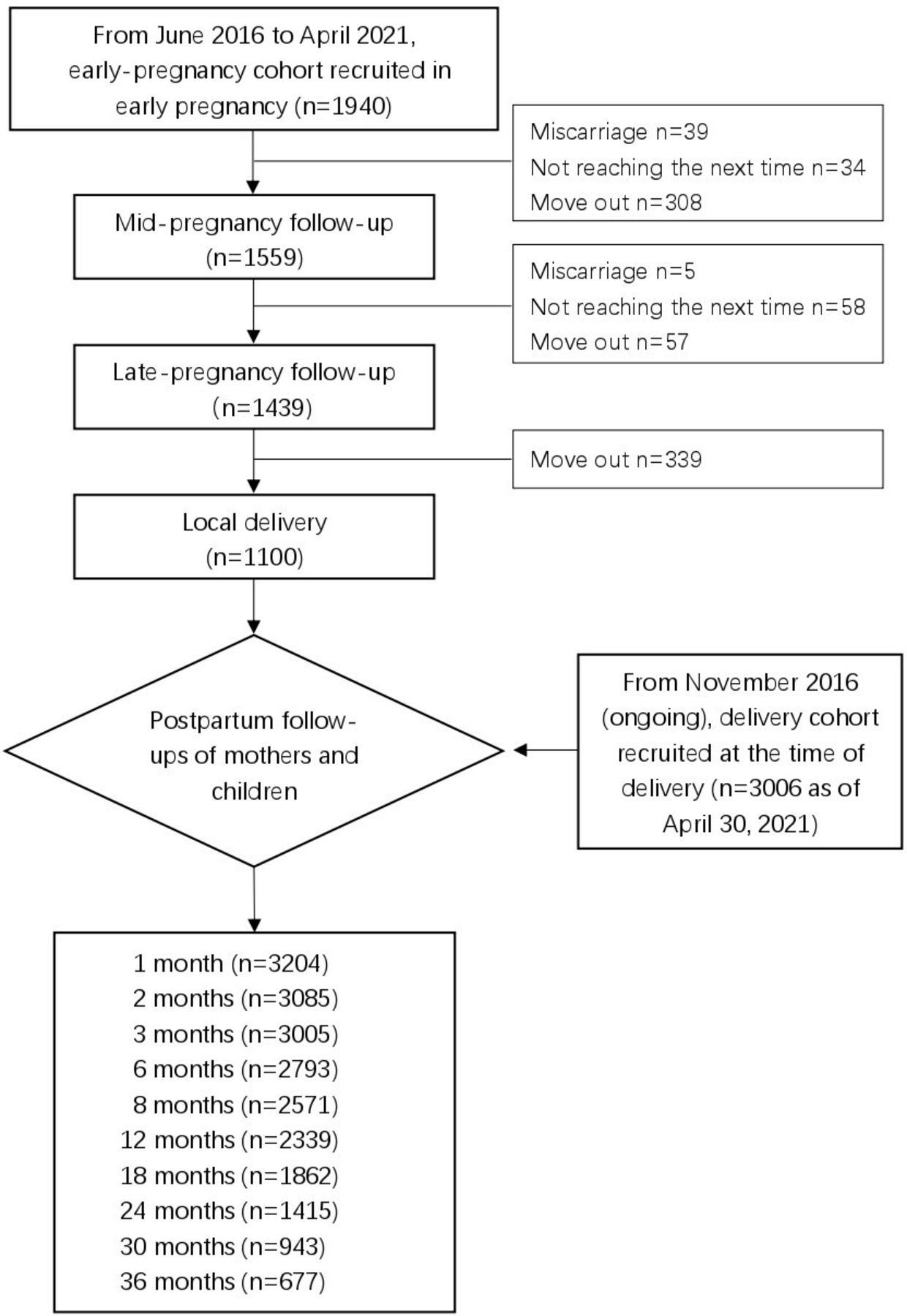
Participants were recruited from May 2013 to December 2017 in Taicang, and from June 2016 to December 2021 in Wuqiang. Pregnant women less than 16 weeks of gestation were invited to participate in the early-pregnancy cohort at both study sites. A delivery cohort was additionally set up in Wuqiang, and pregnant women coming to the Wuqiang County Hospital for delivery were invited to participate in the delivery cohort. We compared data from the two early-pregnancy subcohorts for differences in maternal and childhood nutrition and health at the two study sites. Figures 1 and 2 illustrate the enrolment and follow-up schedule of the study in Taicang and Wuqiang, respectively.

Participant recruitment and follow-ups in the TAWS Taicang subcohort. TAWS, Taicang and Wuqiang Study.

{kind=link}
{kind=link}
Participant recruitment and follow-ups in the TAWS Wuqiang subcohort (ongoing, data presented reflecting study period up to 30 April 2021). TAWS, Taicang and Wuqiang Study.
Participants
Participants were recruited at two stages: (1) early pregnancy (n=4035, early-pregnancy cohort) and (2) during delivery (n=3006, delivery cohort, Wuqiang site). Pregnant women coming for prenatal care were considered potential participants and were approached by trained doctors or nurses for eligibility screening. They were eligible if they: (1) are aged 18–45 years, (2) are less than 16 weeks of gestation, (3) had no history of recurrent abortion, (4) self-reported to be overall healthy without significant medical history (ie, hypertension, diabetes, mental disorders, cancer and other malignant diseases), (5) plan to receive prenatal care and deliver at local hospitals, (6) plan to stay in Taicang/Wuqiang in the next 4 years, (7) are willing to cooperate, (8) are able to write and communicate well. For the delivery cohort in Wuqiang, pregnant women coming for labour were approached and screened by nurses before delivery, with the identical eligibility criteria outlined above, except (2) and (5). Women who agreed to be enrolled in the study provided written informed consent.
For participants in the early-pregnancy cohort, baseline data were collected using questionnaires at enrolment, including information on general characteristics of the pregnant women and their husbands, pre-pregnancy dietary and supplementary intake, pregnancy history and health history. For participants in the delivery cohort, similar baseline data were collected except pre-pregnancy dietary intake.
Cohort follow-up and data collection
Pregnant women received one face-to-face visit at outpatient clinics in each early pregnancy, mid-pregnancy and late pregnancy. Dietary intake was collected using 3-day food records; information on supplementary intake, physical activity (by mobile monitoring devices or self-reported), depression scale, and symptoms or medicines used during pregnancy was queried too. Doctors administered physical and obstetric examinations to check the health status of the mother and the development of her fetus. Twenty millilitres of urine samples and 5 mL of venous blood were collected from mothers at each follow-up during pregnancy at the Wuqiang site (table 1).
Description of data collection methods and time points in the TAWS*
During the delivery phase, pregnancy outcomes (eg, gestational week at delivery, delivery mode, gestational diseases, postpartum haemorrhage, birth weight and length of the newborn, Apgar score) were extracted from medical records. We collected maternal venous blood (5 mL) and neonatal cord blood (5 mL) in both Taicang and Wuqiang. We additionally collected maternal urine (20 mL), placenta (four sites), umbilical cord (3 cm) and meconium (2 g) at the Wuqiang study site (table 1).
After delivery, mothers were followed 7 times in Taicang and 10 times in Wuqiang. Information on dietary intake, supplementary intake, physical activity and mental health was self-reported; and anthropometrics were measured on-site. Fasting venous blood (5 mL) and breast milk (whole milk from one breast using a portable automatic breast pump) were collected from mothers by nurses. Sampling tubes for urine (20 mL) and stool (2 g) were distributed to the mothers, and they were instructed by doctors to collect, store and carry the samples to the clinics at the designated follow-up visits as shown in table 2.
Data collection after delivery in the TAWS*
After birth, children were followed 9 times in Taicang and 10 times in Wuqiang (table 2). General health, growth and motor development were assessed by doctors; child feeding practice (eg, breast feeding, formula, complementary feeding and supplementary intake), dietary intake (using FFQ or 3-day food records) and disease occurrence during the previous 14 days were retrospectively recalled by the caregivers. Samples of blood (5 mL), urine (10 mL) and stool (2 g) were collected at some visits as shown in table 2. To assess child development, the DQ test using the Gesell assessment was administered for a part of children aged 18 and 24 months in Wuqiang.
Biological sample storage and analysis
Blood, stool and breast milk samples were separately stored at −80℃, and urine samples were stored at −20℃. Samples of placenta and cord were fixed in neutral buffered formalin, embedded into wax blocks and stored at room temperature. Levels of vitamins, minerals and metabolites were measured by mass spectrometry. Blood glucose, lipid and haemoglobin were analysed by an automatic biochemical analyser. Microbiome was analysed by the Illumina Hiseq2500 platform. Laboratory quality control materials were run at the beginning and during sample testing.
Compliance promotion
We adopted five strategies to promote participant compliance. First, the two study sites had established standardised follow-up procedures according to the local routine healthcare schedule, which lowered the participants’ burden of transportation and time. Second, all hospitals and health centres worked with the same electronic platform for routine care and follow-up, which has an alarm system to remind doctors to collect data for the study as long as the participants came for care. Third, doctors scheduled appointments for the subsequent follow-up visits via the telephone and informed participants of the contents ahead of the visits. For mothers and children who failed to follow up on time, doctors would call again to make an appointment within a month. Fourth, the principal investigators documented all the issues and provided relevant updated training and feedback to doctors at the regular training sessions every 2–3 months. Fifth, doctors provided mothers or child caregivers with instructions on dietary intake and child feeding practice based on results of physical examination, biochemical testing and dietary evaluation, which would benefit the participants.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research. All participants were informed that the data from this study were used only for research purposes. There were no plans to disseminate the findings to the participants.
Findings to date
Baseline characteristics
The early-pregnancy cohort in Taicang and Wuqiang enrolled 2095 and 1940 women, respectively. Based on data from the early-pregnancy cohorts, the two study sites included pregnant women with different profiles, acknowledging the demographic, health-related and culture-related differences in regions of China as outlined in the TAWS-specific aims. Compared with the study participants in Wuqiang, participants in Taicang were younger and more likely to be enrolled at an earlier gestational age, be primiparas, have a lower pre-pregnancy body mass index, be workers or office clerks and have higher education and higher household income (table 3).
Baseline characteristics of participants in the early-pregnancy cohort of the TAWS*
Gestational diabetes mellitus and metabolomics
Metabolites of mothers and newborns were compared between those diagnosed with gestational diabetes mellitus (GDM) and those with normal glucose.26 Nearly 1000 small molecular metabolites were assessed, and concentrations of 30–40 serum metabolites were different in early pregnancy, second trimester, third trimester, and in umbilical cord blood between women with GDM and those with normal glucose. These results suggested abnormal metabolism occurred through gestation in mothers and their newborns.
Folic acid and birth weight
We analysed the association between folic acid levels during early pregnancy with newborns’ birth weight.27 Median concentration of serum folic acid was 12.3 ng/mL for pregnant women at an average of 13.7 weeks of gestation. There was no association observed between serum folic concentration and newborns’ birth weight. However, maternal serum folic concentration above 14.5 ng/mL was associated with a lower risk of delivering small-for-gestational-age newborns (OR=0.08, 95% CI: 0.01 to 0.61).
Future plans
The TAWS is currently ongoing. Data from the cohort are being collected, processed and cleaned. The association between maternal nutrition and the health of their offspring will be examined at various follow-up visits. Biomarkers will be analysed to assess the associations between early-life nutrition and child development, immunity and health. Strategic recommendations for optimal infant feeding practices, obesity prevention and routine healthcare items will be developed and proposed based on the findings from the study. Children in this prospective cohort study will be followed up once a year until the age of 12 years to further examine the relationships between early-life nutrition and children’s long-term development and health.
Strengths and limitations
Strengths of the TAWS included detailed data on early-life exposures, particularly nutritional information, frequent follow-ups and a wide range of biospecimens available for exploring potential mechanisms of early nutrition on children’s growth and health. Of particular importance, the two study sites had different population characteristics: Taicang is economically more developed and located in southern China, whereas Wuqiang is relatively less developed compared with Taicang and located in northern China; the two study sites, therefore, represent participants with different geographical and cultural profiles, aiming to better reflect and acknowledge the diverse dietary and lifestyle patterns in China. In addition, given the overall economic status of Wuqiang as less developed, nearly half of the pregnant women in Wuqiang did not receive prenatal care; as a result, we established an early-pregnancy cohort and a delivery cohort to better represent profiles of the local pregnant women.
This study has several potential limitations. Similar to other Chinese pregnancy or birth cohorts, generalisability to the diverse Chinese population is a concern. However, our study population’s profile was in general comparable with obstetric characteristics reported in earlier studies.22 28 Second, we had some participants lost to follow-up, who might not be comparable with the participants who remained in the study. Baseline characteristics will be compared between subjects who remained in the cohort and those lost to follow-up to assess the degree of concern due to loss to follow-up. Reasons for loss to follow-up, if related to outcomes yet not accounted in the analysis, might lead to bias in estimating the associations of interest. Third, we prioritised collecting venous blood samples from participants at the follow-up visits, which, under some circumstances, was not feasible, especially for children; we attempted to collect peripheral blood under such circumstances, which may limit the understanding of children’s micronutrient status. Fourth, we did not record the number and the specific reasons for pregnant women who did not meet the inclusion criteria or who were unwilling to participate in this study. Based on our communication with doctors during the training sessions, the main reason for not meeting the inclusion criteria was exceeding the gestational age criteria for the early-pregnancy cohort, and some pregnant women were unwilling to participate because of the large content and the long duration of the study.
Collaboration
Data of the TAWS are not openly available yet. Researchers who are interested in potential collaboration should contact the principal investigator, Jianqiang Lai (jq_lai@126.com), to submit a research plan for evaluation by the Ethical Review Committee of NINH.
Data availability statement
Data are available upon reasonable request. Data are available on reasonable request, including anthropometric data and micronutrient status data of mothers and children.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethical Review Committee of National Institute for Nutrition and Health, and Chinese Center for Disease Control and Prevention (approval numbers: 2013-001 and 2016-014). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to all the collaborating organisations and staff of the TAWS whose hard work has made this study possible. We would like to thank the 22 community health centres in Taicang for their follow-ups during pregnancy and post partum, and 5 hospitals in Taicang for the follow-up during delivery. We would like to thank Wuqiang Maternal and Child Health Care Hospital and the eight township health centres for follow-ups during pregnancy and post partum, and Wuqiang County Hospital for the follow-up at delivery. We would like to thank all the study participants and their families for their voluntary participation and ongoing support for the TAWS.
References
Footnotes
JW, YD and JY contributed equally.
Contributors SY, YD, JW, ZY and JiL designed the cohort. JuL, FL, PZ, CL, YZ and XG coordinated the fieldwork and supervised data collection. JW took charge of the training and quality control in the Taicang subcohort, and YD was responsible for the Wuqiang subcohort. JW and YD performed data process and statistical analysis. JY, YD and JW wrote the manuscript. ZY, CY and JiL reviewed the manuscript. JiL was responsible for the overall content as the guarantor. All authors have read and approved the final version of the manuscript.
Funding This study was funded by the National Health Commission of China (2017-2021), UNICEF China office (12241, 12217) and Taicang Health Commission (2016-2020).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.