Article Text

Abstract
Objective Bangladesh is currently undergoing an epidemic of road traffic crashes (RTCs). In addition to morbidity and mortality, the economic loss from RTC as per cent of gross domestic product is comparatively higher than in countries with similar socioeconomic conditions. However, trauma care remained poorly developed as a specialty and service delivery mechanism. This study aimed to examine the current situation of in-hospital trauma care after RTCs to inform the design of a comprehensive service for Bangladesh.
Design, setting and participants This qualitative study attempted to elicit stakeholders’ perceptions and experiences of managing RTCs through in-depth interviews and focus group discussions. Three districts and Dhaka city were selected based on the frequency of occurrence of RTCs. Fifteen in-depth interviews and 5 focus group discussions were conducted with 38 RTC patients, their relatives and community members in the catchment areas of 11 facilities managing trauma patients. Key informant interviews were conducted with 21 service providers and 17 key stakeholders/policy-makers.
Results Hospital-based trauma care was generally poor in primary and secondary-level facilities. There was no triage area or triage protocol in the emergency rooms, no trained staff for trauma care, no dedicated RTC patient register and scarce life-saving equipment. Only in Dhaka-based tertiary hospitals was trauma care prioritised. These hospitals follow Advanced Trauma Life Support guidelines and maintain an RTC logbook. Emergency diagnostic services were not always available in the hospitals. Most RTC patients were males; the female participants were additionally vulnerable to physical and mental trauma. Affected people avoided taking legal action considering it a lengthy, complicated and ultimately ineffective process.
Conclusion The trauma care services currently available in the studied health facilities are very rudimentary and without the necessary human and financial resources. This needs urgent attention from policymakers, programmers and practitioners to reduce morbidity and mortality from the current epidemic of RTCs in Bangladesh.
- Road traffic injury
- Trauma care
- Emergency services
- Bangladesh
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study included diverse respondents and used data triangulation.
It shed light on road traffic crash (RTC) patient experiences and service availability across different levels of facilities.
A limitation is that retrospectively collecting data from RTC patients can cause recall biases and lead to incomplete cost information.
Recent RTC patients were unable to reflect on their coping mechanisms due to ongoing rehabilitation.
Background
Road traffic crash (RTC) is the world’s eighth leading cause of death, with one person dying every 24 s.1 It is one of the top three causes of death among people aged 5–44 years and the leading cause of death among those aged 5–29.2 3 The low-income countries bear the burden of these deaths, accounting for 13% of all deaths despite owning only 1% of registered vehicles. RTCs disproportionately harm the poor and are also a source of poverty for many households.1 4 Moreover, RTCs significantly impact these households’ health-related quality of life because they have physical, psychological and financial implications.5 6 Thus, the problem has evolved into a public health issue. The United Nations General Assembly declared a Decade of Action for Road Safety 2011–2020 to reduce, mitigate and reverse the situation.1 Additionally, the health-related global goal for sustainable development (3.6) aims to reduce fatalities and injuries by half by 2030.1
Bangladesh is currently experiencing an epidemic of RTCs with a very high fatality rate (100 deaths per 10 000 motor vehicles) compared with the proportion of vehicle ownership.7 RTC-related injuries were the ninth-leading cause of inpatient admission in all government hospitals for persons over 5 in 2017. An estimated 25 023 (95% CI 20 799 to 29 185) deaths occurred from RTCs in Bangladesh in 2019, and the economic loss is estimated to be around 2%–3% of gross domestic product, a significant development burden.1 The latest Global Status Report on Road Safety registered some improvements for Bangladesh concerning safer roads and mobility and safer vehicles but noted poor performance in areas like gathering crash data, safer road users and post-crash care.1
In Bangladesh, two-thirds of all RTC fatalities occur during patient transport from the crash site to the health facility, and three-quarters do not receive any prehospital trauma care.8 These factors that impact trauma patients’ survival outcomes are still not prioritised in Bangladesh. While the country has made considerable gains in child and maternal survival, maternal mortality and infectious diseases, trauma care is less developed as a specialty and healthcare service.9 For designing and developing a comprehensive trauma care system following RTCs in Bangladesh, detailed information on currently available hospital-based post-crash care services in the country is essential. This study aimed to qualitatively assess the provision of trauma care in healthcare facilities for RTC patients in Bangladesh, elucidating the non-numerical aspects. This research aims to inform the development of a comprehensive trauma care system in accordance with scientific rigour.
Methods
Study design
This is a qualitative study to elicit experiences and perspectives of the RTC victims through in-depth interviews (IDIs) and focus group discussions (FGDs) with road injury patients, including their family members and members of the catchment community. In addition, the experiences and perspectives of the key stakeholders, such as trauma care providers and others in policy and practice, were also sought through key informant interviews (KIIs). Purposive sampling followed by snowball sampling techniques was applied to recruit study participants. Data were collected between February 2020 and June 2021 in two phases because of the interruption caused by the pandemic.
Study sites
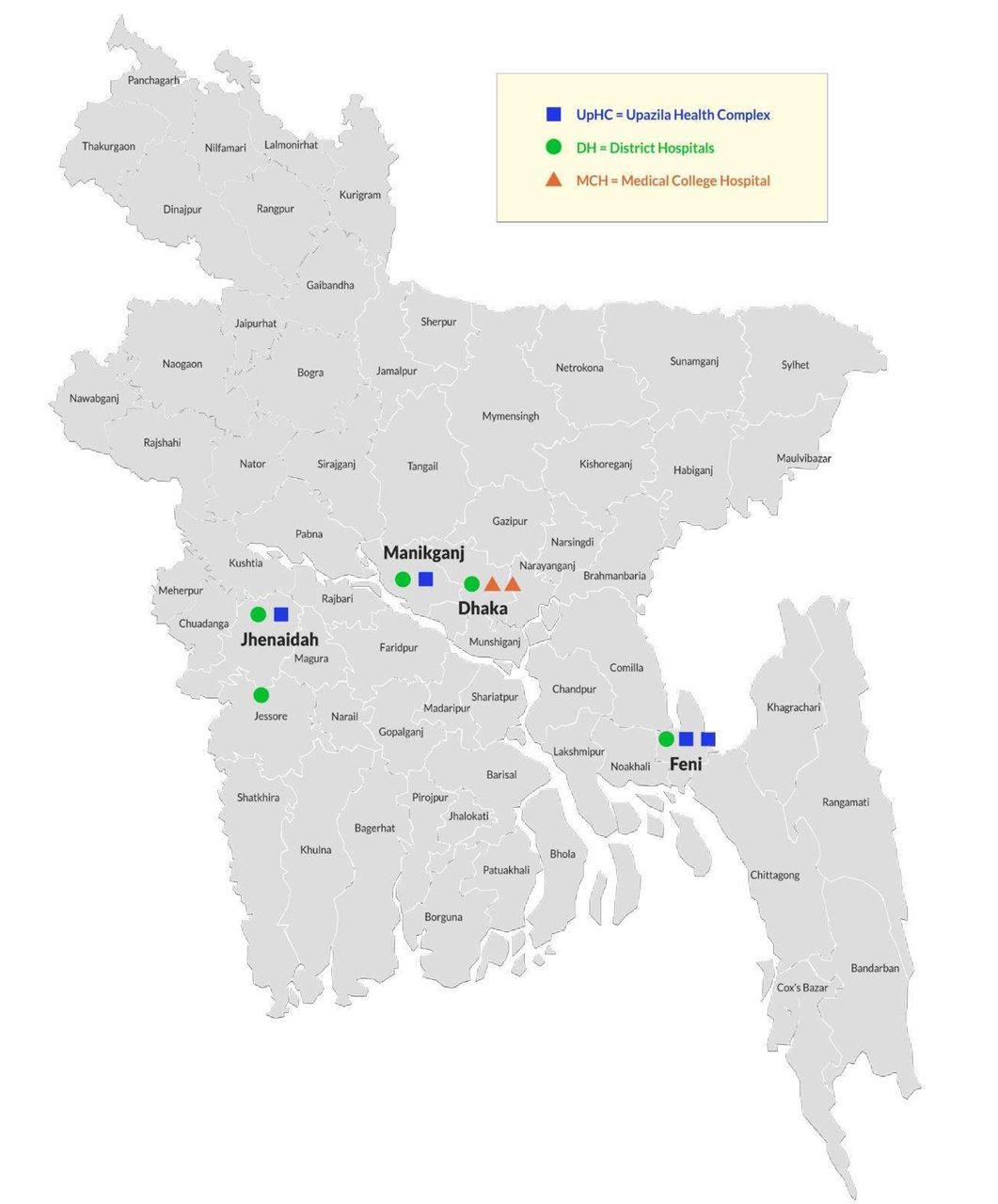
Data were gathered from health facilities of four districts in Bangladesh situated along the highways. These are Dhaka, Manikganj, Feni and Jashore. These sites were purposively selected based on the frequent occurrence of RTCs. A total of 11 facilities from the primary to the tertiary level were chosen as the study sites (figure 1).

Different tiers of health facilities and the number of selected facilities from each site.
At the district level, mainly the primary (upazila health complexes, UpHCs) and secondary (district hospitals, DHs) level public sector health facilities were included. In Dhaka, one secondary and two tertiary health facilities (including one private tertiary facility) in the south city corporation area were selected to understand the urban context (big city, densely populated) in this study. Figure 2 shows the locations of the four selected study sites on the map.

{kind=link}
{kind=link}
Map showing different study sites from the selected districts and Dhaka City.
Study population
The study sample was recruited from the supply and demand sides to comprehensively understand the hospital-based trauma care situation (table 1). On the demand side, the study population included representatives of the ‘catchment community’, RTC patients or their relatives (n=58). Fifteen IDIs were conducted from our study sites.
Total no of interviews and different types of respondents participated in the study
The inclusion and exclusion criteria for the selection of the different participants were as follows:
RTC patients/victims
Inclusion criteria
Adults aged 18 years and above who had experienced RTCs were eligible.
Only RTC patients/victims residing in the specified study sites were included.
Participants had to seek care from formal healthcare facilities.
Exclusion criteria
Individuals below 18 years of age who had experienced RTCs were not included.
Victims who did not seek care from the designated formal healthcare facilities were excluded.
Accidents that did not occur within the study sites were not considered for analysis.
Relatives
Inclusion criteria
Close relatives or legal guardians (parents, spouses, siblings) residing in the same household who are well-informed about the patient’s road injury.
Relatives must be 18 years of age or older.
Participants must have been either present at the scene during the RTC or involved in taking care of the patients during and after the accident.
Exclusion criteria
Relatives who do not have a clear understanding of the patient’s RTC.
Those who did not participate in taking care of the patients or did not witness the entire incident were excluded.
People under the age of 18 was excluded from the study.
Community people
Inclusion criteria
Local people or bystanders who have experience observing multiple RTCs.
Individuals with experience in transferring RTC victims to hospitals.
Participants must be 18 years of age or older.
Exclusion criteria
Those who have never had any experience observing RTCs at the scene.
People who had never assisted in transporting RTC victims to hospitals.
Participants below the age of 18.
Service providers
Inclusion criteria
Formal service providers employed by either private or public facilities.
Service providers who deal specifically with RTC cases.
Providers who were then posted and serving in the selected facilities.
Exclusion criteria
Informal caregivers were not included.
Providers who did not handle RTC cases.
Providers who were not posted or serving in the selected facilities during the data collection.
Stakeholders and/or policy-makers
Inclusion criteria
Those actively participating in RTC-related activities, such as raising awareness, preventing RTCs or providing financial support to victims and their families.
Professionals engaged in policy-making, especially in the context of RTCs.
Participants must be 18 years of age or older to be eligible.
Exclusion criteria
Those not actively engaged in RTC-related activities.
Professionals involved in policy-making unrelated to RTCs.
Participants below the age of 18.
Additionally, 5 FGDs were held with 7–10 participants in each. On the supply side, the study population included healthcare service providers from selected health facilities (n=21) and relevant key stakeholders and policy-makers (n=17). Key stakeholders such as local and national level security and healthcare administrators and policy-makers were selected purposively and through a snowball technique. The study team conducted KIIs with the respondents at their workplaces and at a convenient time.
Tools development
A set of guidelines for KIIs, IDIs and FGDs were developed to elicit participants’ in-depth perceptions, opinions, procedures and observations about RTC-related services as outlined in the study objectives. All the guidelines were developed in English and then translated into Bangla. Tools were revised and refined after pretesting on a small sample and used for field data collection.
Recruitment and training of field data collectors
Experienced research assistants with knowledge of qualitative data collection methods were recruited through a competitive process, and a 3-day training was organised for the team before deployment in the field. The training covered topics on the RTC situation in Bangladesh and the need for improving post-crash trauma care in the country in the context of WHO guidelines, the current scenario of trauma care in the health facilities, qualitative methods and tools for IDI/FGD/KIIs, rapport-building techniques, etc. Didactic lectures, role-playing and field practice methods were combined for training. Two teams were organised for data collection, each consisting of two research assistants, led by a senior researcher.
Data collection and quality control
IDIs were conducted with RTC patients/their relatives in the community at a convenient place and time. A prescheduled appointment list was used to conduct KIIs at a place and time convenient to the respective key informants (KIs), with each interview lasting from 60 to 90 min. FGDs were conducted with support from the local community in a common courtyard area. Participation in the interviews and FGDs was completely voluntary. Each team was led by an experienced supervisor who guided data collection and cross-checked the quality of the collected data. The team members used to have a group meeting at the end of the day to check for consistency of data collected and any missed information. The senior researchers regularly evaluated interview transcripts and recordings for completeness, accuracy and reliability, using a quality control checklist.
Data analysis
We undertook a thematic analysis on this set of qualitative data.10 Data analysis was conducted in three stages. In the first stage, verbatim transcripts were prepared in Bangla. We used a standard template to prepare the transcript and maintain consistency. To minimise recall bias, audio records (of those giving consent) and handwritten notes were used to prepare transcripts on the same day. Each transcript was then reviewed and revised by the team members the following day to address any issues or corrections.
In the second stage, the Bangla transcripts were translated into English by the first (SNBKT) and another researcher (not an author). The researchers diligently reviewed and cross-checked each other’s translations to ensure accuracy and appropriateness, thereby maintaining the integrity of the translated content.
In the third stage, a list of a priori codes were developed based on the guidelines. Based on the literature review,1–5 7 8 the guideline was prepared, and then we have selected the following a priori codes for the analysis:
Availability of trauma care services in healthcare facilities.
Expenses associated with RTC care.
Physical and mental consequences arising from RTCs, including rehabilitation.
Post-RTC legal issues.
These codes were applied to the transcripts, and additional inductive codes emerged during the reading and rereading of the text, which were also included in the analysis. The following are examples of emerging codes in this study:
Gender dimension.
Variations in RTC services between day and night shifts.
Coping mechanisms for RTCs.
We used a template to organise and analyse the data according to themes and subthemes, informed by the prior scoping review on the topic.1–5 7 8 The manuscript included illustrative quotes to provide a vivid representation of the real-life situation.
Patient and public involvement
The design, conduct, reporting or dissemination of the results of this study were not done with the involvement of the general public or/and patients.
Results
Sociodemographic characteristics of the community respondents
A total of 53 community respondents (RTC vistims/patients and their family members/nearest neighbours) from these four study sites participated in this qualitative study. Among the community participants, the majority (70%) were male, aged between 18 and 70 years (mean age: 32), and the majority (87%) were married. About one-third (34%) had no formal education, and their monthly family income ranged from BDT5000 to BDT30 000, with a mean income of BDT14 000. Nineteen per cent of the RTC victims were transport workers (drivers/helpers of CNG-a three-wheeler transport, van, rickshaw, bus, etc), and most crashes occurred in urban areas (64%) (table 2).
Sociodemographic profile of community respondents (n=53)
Trauma care services available in the health facilities
Most RTC patients first sought care from nearby health facilities. The rural RTC cases first visited the UpHCs. On the other hand, people living in urban areas or those who experienced road traffic accidents in urban areas outside Dhaka first visited the district/general hospitals or private facilities. Findings revealed a lack of trauma care services in the emergency or inpatient facilities, including the absence of any triage facility on arrival of the RTC patients. In the UpHCs, the service providers mentioned a few emergency beds and some equipment for basic wound care, but they had no advanced equipment. Sometimes, the UpHC and DH emergency rooms were crowded due to mass casualty events, and the lack of dedicated units and providers resulted in RTC patients having to wait while other seriously ill medical patients were being attended to. Although people used to visit UpHCs for minor injuries (eg, abrasions, bruises, tears or superficial cuts), no service provider was available to attend to them. In most cases, patients were referred from the UpHCs to the DHs (online supplemental figure 1). The RTC patients or their relatives/attendants expressed dissatisfaction with the care provided at the UpHCs:
Supplemental material
I didn't like the services provided by the UpHC providers. There was a lack of equipment and Physicians as well… I only received the first aid care from there and was referred to the district hospital [Male RTC victim, 34 yrs. old]
Service providers at DHs stated that they had an emergency unit and could manage RTC patients. The RTC patients shared the same space with other medical emergency patients, and these patients were admitted to the surgery or the orthopaedics department if needed. However, major surgeries could not be done in the DHs due to a lack of essential equipment, diagnostics and medicines (online supplemental table 1).
Supplemental material
Trauma care was mainly concentrated in the secondary and tertiary level public sector hospitals in the big cities; however, they, too, had varied resource shortages, including essential medicines. A lack of necessary knowledge and skills among the emergency-room staff and doctors was observed. Moreover, there was a shortage of skilled staff at all levels:
None of us is trained in trauma care …some of our EMOs and surgery consultants have completed FCPS in surgery, where they learnt how to manage the RTC patients …but no specific course or training was received by them…another challenge is we have a shortage of workforce. [KII_ Service Provider]
Generally, clinical protocol or standard guidelines such as Advanced Trauma Life Support (ATLS) were only practised in public tertiary-level hospitals. Emergency room staff reported a shortage of clinical skills to manage life-threatening injury situations. The DHs had X-ray, and laboratory facilities through X-ray service were limited or unavailable after office hours. Timing of service delivery posed a barrier to accessing emergency care:
I needed an emergency X-ray test in the evening right after the crash happened….but no X-ray services were available at DH after office hours, and the emergency doctor told me to get that from a private facility. [Male RTC victim, 45 yrs. old]
In addition, post-crash rehabilitation service was found to be almost non-existent except in tertiary-level facilities. Findings also reveal an absence of RTC surveillance and record-keeping in health facilities. In the UpHCs, RTC cases were recorded in the emergency logbook along with other emergency cases, while in the DHs, a separate logbook was maintained for all types of injury-related causalities, including the RTC cases. The private tertiary facility did not have RTC case records/logs. The public tertiary-level hospital only maintained a dedicated register book for RTC patients. The UpHC, DH and tertiary hospitals reported RTC cases along with other cases to the DGHS every month (online supplemental table 2). The KIs supported the findings and informed that emergency care was still not developed as a specialty in the undergraduate and postgraduate medical education curricula.
Supplemental material
Gender dimension
Some of the female victims stated they did not get any attention from local people. Instead, they perceived that they were actively overlooked because of their gender:
The bike left the spot right after the accident… my leg was under an auto-rickshaw, and the driver fell and was injured. I noticed that some people were helping the driver but not me, because I am a female… I felt so helpless at that moment. [Female RTC victim, 31 yrs. old]
Female victims of RTCs, burdened with household responsibilities, were stressed and concerned RTC about their families, health and financial support. For example, one of the female victims (26 years old now) had a head injury from a road traffic accident (10–12 years ago), lost her memory and ‘could not’ remember anything except that her parents had to take a large loan from relatives for her treatment. She lost her parents a few years after the accident, and her husband also passed away 2–3 years ago. Her neighbours, in an FGD, reiterated her poor state:
She lives alone here… if someonegives her something, she eats or buys some medicines or clothes … no one is there to help her…we, the neighbours, try to help her, but it’s also not always possible. [Female victim’s neighbours] [The victim (26 yrs. old lady)] was nodding her head with the response and constantly crying during the FGD]
Apart from the female RTC patients, the female family members of both male and female victims (mothers/sisters/wives) also became vulnerable as they had to take care of the RTC patients on top of their daily household chores, including income-earning for the household.
Cost of RTC care
At the UpHCs and DHs, lab investigations were free of cost, and no emergency fund was available at the UpHCs for such RTC victims. However, DHs had few earmarked funds and social welfare funds which were used to support RTC patients in some cases. According to the community respondents, the cost of treatment varied based on the type of facility, whether public or private. For the latter, the cost was much higher. Respondents who received treatment from DH hospital found it reasonable unless a major surgery was done, or a blood transfusion was needed. When the patients were referred to the tertiary hospitals in Dhaka for major surgery or orthopaedic surgery, the cost of treatment becomes quite high, ranging from BDT50 000 - to a few lakhs at a time as they had to pay for medicines, diagnostics, and some surgical materials for orthopaedics surgery:
I had to spend a total of BDT 1 lakh and 20 thousand on the operation, including the cost of medicines, rods, and other expenses. [Male RTC victim, 18 yrs. old]
Respondents who received treatment from private hospitals had to spend quite a few times higher than those receiving treatment from public facilities. Apart from immediate expenditures, the RTC patients had to undertake out-of-pocket (OOP) expenditures for continuous care and follow-up. Other than the direct treatment costs, the patient or family had to manage attendees'/caregivers’ costs while staying in the hospital. Sometimes, the family had to undergo an extreme financial crisis and sell their property, land, domestic animal and jewellery to raise the cost of treatment. Still, others had to borrow from family members, relatives, friends, etc, to continue treatment.
Regarding the cost of RTC trauma care, service providers and stakeholders echoed patients’ opinions. They mentioned that although the cost of services in the public facility seemed relatively low, it increased with the severity of the injury and the need to spend on medicines, diagnostic tests and surgery:
Although the emergency ticket is only BDT 10 at the public facility, I had to purchase a lot of medicines outside and spent a huge amount on diagnostic tests. I even needed to take a loan to continue my treatment. [Male RTC victim, 54 yrs. old]
Physical and mental health issues due to RTCs, including rehabilitation
Some of the respondents were physically disabled RTC patients, and some had difficulties in movement since the incident. Several respondents had lost their family members due to RTCs. Some of the RTC patients also developed anxiety and fear of road travel. Throughout these sufferings, their family remained the main source of support:
I lost my hand, cannot earn like before, and I cannot eat good food with family…. When people ask me where is your hand? It hurts me, and I am mentally upset due to this reason…and now, if I have to take some loan from anyone, they cannot trust me because I lost a hand; how can I earn. [Male RTC victim, 36 yrs. old_FGD1]
Physical disability limited their livelihood and income-earning options, and they had to change professions. Those who were driving eventually had to give up the job. Key stakeholders mentioned that only a few organisations did provide some financial support to disabled RTC patients, which was never enough. They also mentioned that disabled patients were not only a burden for the family but also a burden for the entire country.
Post-crash legal issues
The KIs mentioned that the RTC investigation procedures are lengthy and complicated. The RTC patients/community respondents who faced RTC did not file any legal case against the accused as they found it complicated, lengthy and expensive. The duration of the investigation and legal process varied case by case; filing a case and getting a decision can take a few months to several years, as the KIs stated. Similarly, the community respondents doubted whether they would get support from law enforcement authorities as, in many cases, the accused vehicle (truck) driver had a good relationship with the local police. To quote:
About 90% of the populationdo not want to file a case for road traffic injury. There is no outcome of the case; rather, the people must undergo harassment due to filing these cases. [KII_ High Govt. Official]
Community respondents preferred to use their money better for treatment purposes instead of going through this long process. According to KIs, many facilities, especially the private sector facilities, did not receive RTC patients to avoid legal procedures and police interrogation. This is a significant challenge for the bystanders and the law enforcement authorities while transporting the victims to facilities for emergency care. Also, the central-level authorities mentioned GoB mandatory rules to provide emergency care to any patient coming to the private facility. However, it did not happen in reality.
Discussion and recommendations
This qualitative study attempted to explore stakeholders’ perceptions and experiences regarding the in-hospital management of RTC patients/victims in order to inform the design of a trauma care system for Bangladesh. IDIs and FGDs were conducted with RTC patients, including relatives of the patients and members of the catchment community, and KIIs with stakeholders in policy and practice. Findings reveal a poor state of trauma care services in the studied primary and secondary health facilities with a shortage of skilled human resources, necessary equipment and financial resources. No unique trauma protocol was followed in these facilities, including inadequate documentation of RTC patients for evidence-based decision-making. The implications of the findings for designing a comprehensive trauma care system are discussed.
This study’s findings reveal that RTC cases were initially transferred to a primary or secondary-level health facility close to the site of accidents. However, most cases ended up being referred to the tertiary level facilities in the big cities. It was disheartening to see that neither the emergency room nor the in-patient facilities had a designated trauma care team or a triage facility. No trained trauma care provider was available, and no clinical protocol or standard operational procedure (SoP) was followed in these facilities to ensure essential trauma care. However, as per the guidelines of the International Federation for Emergency Medicine, it is expected that trained personnel in the emergency departments would prioritise patient-centredness, timeliness and expertise in decision-making while being supported by well-designed systems, processes, diagnostics, appropriate equipment and facilities to provide effective acute care.11 Only the government tertiary-level hospitals had a dedicated casualty ward and a trauma protocol/SoP in place (ATLS). The lack of a trauma care team and a consistent treatment protocol are the areas of concern in the different LMICs.12 13 However, evidence shows that implementation of a standard trauma care protocol reduced in-hospital mortality (eg, among RTC patients with severe traumatic brain injuries) and decreased the length of hospital stay at a teaching hospital in a low-income middle-income country.14 The same is true for triage facilities to categorise RTC patients based on the severity of the injury. In a study from Afghanistan, triage levels were found to correlate well with mortality outcomes, for example, none of the patients triaged as green died or was admitted to the ICU, whereas 90% of patients who died were triaged as red.15 The study observed that the majority of the RTCs occurred in metropolitan locations, and most of them occurred during the daytime. This is consistent with another study from Bangladesh, which found that the majority of RTCs occurred in the morning and urban areas.8
Findings reiterate the need for maintaining an RTC surveillance system at each level of health facility to produce disaggregated data on RTC cases, as UpHCs and DHs usually did not maintain a separate register for these patients. The same is true for the tertiary level private facilities. This agrees with what was found in a study from India.16 The importance of a trauma registry with a potential role in filling a critical gap in injury data for health-related outcomes cannot be overemphasised. Also, it has been observed that a comprehensive TR can aid in the improvement of RTC treatment quality by identifying gaps in the trauma system and opportunities for practice improvement.17 The problem of time-consuming manual documentation by the busy emergency room staff can be lessened more efficiently by an electronic data registry system (e-trauma registry), as found elsewhere.18 19
The RTC patients have a gender dimension similar to global findings: there are more male RTC patients compared with females (WHO, 2022). A recently conducted study in Bangladesh also showed the number of female RTC patients to be less than the number of males.8 Females suffered more from RTCs and faced unique difficulties such as the double burden of caring for the RTC patient and catering to income-earning for the family. Furthermore, the cost of care may be too high in comparison to household income, making treatment of the RTC patient unaffordable.20 The White Paper providing guidelines for the development of International Trauma Systems aligns with The US Trauma System Agenda for the future. It emphasises four fundamental Trauma System components: injury prevention, prehospital care, acute care facilities and post-hospital care. Moreover, it highlights the crucial importance of eight fundamental infrastructure components, including leadership, professional resources, education, information management, finances, research, technology and disaster preparedness/response.21 Bangladesh requires to establish a complete set of guidelines, similar to a ‘White Paper’, to provide a structured and organised roadmap for the gradual development of a practical and effective Trauma System for RTCs, addressing the exact necessities and circumstances of the country’s healthcare system.
Limitations of the study
This study does have a few limitations worth noting. The retrospective collection of data from RTC patients introduces the potential for recall bias, which may affect the accuracy of healthcare-related information gathered from different facilities. Additionally, incomplete cost-related information provided by some patients could restrict the study’s ability to provide comprehensive economic insights. Furthermore, limitations arise from the incapacity of certain patients, who experienced RTCs several days or even months prior, to fully articulate their coping mechanisms due to ongoing rehabilitation.
Conclusions and recommendations
The readiness of the health facilities to receive and manage trauma victims, including RTC victims, varies across tiers and areas, especially at the roadside health facilities. The lack of human resources for health from the grassroots to the top level (eg, physicians, nurses, allied health professionals) with proper training and skills appear to be the most significant barrier to establishing a high-quality trauma care system in the country. Furthermore, trauma and emergency care are still not developed as a specialty at medical school’s undergraduate and postgraduate levels. This is required to produce industry-leading experts and specialists. At the communal level, women are particularly vulnerable to RTCs and require financial and mental health support from the government or non-governmental organisations. Based on the study findings, the following recommendations are made:
Ensure a dedicated trauma team (as part of emergency care) with skilled staff, appropriate and functional equipment and necessary financial resources at all levels in all hospitals from UpHC to district and above (secondary and tertiary care hospitals), formulate SoPs and adopt standard protocols (eg, ATLS) for managing trauma cases, including RTC cases in the emergency rooms, and train the emergency room staff.
Second, arrange emergency/contingency funds for the RTC patients at the hospitals to reduce high OOP and catastrophic expenditure for the victims and their families; mobilise and allocate resources for developing a dedicated post-crash care/trauma care unit/system in the country. Finally, the topic should be included in the health-professional education curriculum, from the undergraduate level to the postgraduate, to produce experts and specialists who can provide leadership to the sector.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Prior approval was taken from the Ministry of Health and Family Welfare (MoHFW) for data collection from the selected health facilities. Ethical approval was obtained from the Institutional Review Board of the BRAC James P Grant School of Public Health, BRAC University, Dhaka, Bangladesh (reference No. 2020-004-IR). Informed voluntary consent in Bangla, including consent to record the conversation, was obtained from all respondents. Moreover, all the participants provided written consent for participating in the study. They were informed about the study’s purpose, process, risk and benefit. Respondents were given a choice to withdraw from the interview at any time during the study if they wanted. Privacy, anonymity and confidentiality were maintained throughout the study and were used for research purposes only.
Acknowledgments
The study team expresses gratitude to the funder (The World Bank) for providing technical support to the team throughout the study period. Researchers extend their thanks to the Field Monitoring Supervisor, Mir Raihanul Islam, and the Research Assistants, including Md. Mehedi Hasan Sarkar, Zarin Tasnim, Md. Nasir Uddin, and Md. Zakir Hossain, for their invaluable assistance in field activities and data collection. Finally, the team conveys their heartfelt appreciation to the study participants, without whom the study would not have been possible to complete.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation: SNBKT, NN and SMA, Methodology: SMA and SNBKT, Data collection: SNBKT and BZI, Formal analysis: SNBKT and NN, Roles/writing—original draft: SNBKT, AM and SMA; Writing—review and editing: SNBKT, AM and SMA, Guarantor- SMA. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests The authors declare that they have no competing interests.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.