Article Text

Abstract
Introduction Child maltreatment (CM) is a complex global public health issue with potentially devastating effects on individuals’ physical and mental health and well-being throughout the life course. A lack of uniform definitions hinders attempts to identify, measure, respond to, and prevent CM. The aim of this electronic Delphi (e-Delphi) study is to build consensus on definitions and types of CM for use in surveillance and multi-sectoral research in the 34 countries in the Euro-CAN (Multi-Sectoral Responses to Child Abuse and Neglect in Europe) project (COST Action CA19106).
Methods and analysis The e-Delphi study will consist of a maximum of three rounds conducted using an online data collection platform. A multi-disciplinary expert panel consisting of researchers, child protection professionals (health and social care), police, legal professionals and adult survivors of CM will be purposefully recruited. We will approach approximately 100 experts, with between 50 and 60 of these anticipated to take part. Participants will rate their agreement with a range of statements relating to operational definitions and types of CM, and free-text comments on each of the statements to give further detail about their responses and areas of uncertainty. Consensus has been defined a priori as ≥70% of the panel agreeing or disagreeing with the statement after the final round. The responses to the open-ended questions will be analysed using a ‘codebook’ approach to thematic analysis, and used to refine the statements between rounds where no consensus is reached.
Ethics and dissemination Ethical approval has been granted from the Cardiff University School of Medicine ethics committee (reference number SMREC22/96). Results will be submitted for publication in a peer-reviewed journal and presented at workshops (including for the participants) and international academic conferences. The Euro-CAN network will also be used to disseminate the results, with results briefings and presentations to key public health and other relevant organisations in the field.
- child protection
- non-accidental injury
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study is using the robust and systematic Delphi method, the gold standard for studying and building consensus.
The study team has conducted detailed background work using different methods to identify the research gaps and areas of focus for this study.
Facilitated by online data collection methods, the study will recruit an international multi-disciplinary expert panel from 34 countries and will include adult child maltreatment (CM) survivors.
Challenges include the fact that different disciplines use their own terminology when discussing CM.
The questionnaire will be administered in English, which is not the mother tongue of most study participants.
Introduction
Child maltreatment (CM) is a serious and complex global public health issue that can have devastating and pervasive effects on individuals’ physical and mental health and well-being across the life course.1 Adverse childhood experiences, including interpersonal violence, are associated with significant health, financial and social costs across European countries,2 yet the costs to society are preventable. Over 55 million children in Europe experience some form of CM every year.3 However, incidence and prevalence estimates of CM vary considerably across studies, contexts and countries, and are likely to be under-estimates.4–9 The United Nations 2030 Agenda for Sustainable Development includes a clear call to eradicate violence against children.1 Consistent measurements of the incidence, prevalence and characteristics of CM are needed to measure progress against this goal, make comparisons across settings, and inform more focused prevention and intervention efforts.10
Several different classification systems for CM have been developed, with each using different approaches, definitions and terminology.10–15 While some of the discrepancies in measurements are likely to be due to different study designs, sampling procedures and methodological approaches, much of the variance can be attributable to differences in definitions and types of CM applied in these systems and their operationalisation.16 17 Inevitably, broader definitions will produce higher estimates and may lead to false positive error, while narrower definitions will produce lower estimates, and may lead to false negative error. Both types of error will have detrimental consequences for children and families. Different sectors involved in child protection practice and research use their own terminology and tend to use differing definitions.17 Definitions can often be non-specific or implicit and operationalisations of important terms and concepts are frequently lacking.17 In addition, the definition and interpretation of CM depends on sociocultural values and norms, which vary within and between countries, and change over contexts and time.18
Both population-based surveys and studies using administrative data suffer from a lack of uniform, consensus-based definitions and operationalisations of CM. This limits communication, and hinders attempts to identify, measure, respond to and prevent CM. It also limits the ability to monitor and compare trends in CM over time, and therefore the effectiveness of intervention and prevention programmes.19 It has long been recognised that common, multi-sectoral conceptual definitions and operationalisations of CM are needed to improve data collection and surveillance of CM across different sectors and countries in Europe.15 Standardised pan-European definitions and operationalisations of CM will allow for comparable epidemiological findings and facilitate implementation of policies and legislation at a European level, thereby improving the likelihood of equitable child protection and support both within and between countries.
Several attempts have been made to define data elements and variables to improve surveillance and ensure consistent measurement of CM across different settings. In three of these, the methods used to develop uniform definitions and data elements included interviewing and consultation with a small number of experts, and in-person meetings, but no formal attempt at consensus building.10 20 21 In addition, two approaches focused on one specific aspect of CM only, with Breiding et al20 focusing on intimate partner violence and Parks and Hill21 examining paediatric abusive head trauma. A further recent study used a modified Delphi method to develop a consensus definition of near-fatal CM for use in practice, policy and research.22 Although this study also focused on one specific type of CM, its results suggest that reaching consensus using a Delphi method is feasible in this field.
In a unique initiative, a consortium of researchers from 10 European countries developed and piloted the CAN-MDS (Coordinated Response to Child Abuse and Neglect via a Minimum Dataset) surveillance system.23 24 CAN-MDS is a public health surveillance mechanism designed to standardise the measurement of incidents of child abuse and neglect and uses a common methodology and definitions across countries and different sectors. Data collection is based on a minimum data set supported by a bespoke toolkit (www.can-via-mds.eu). The current study will build on the experiences and lessons learnt from this ambitious pan-European project.
More recently, UNICEF has developed a statistical classification on all forms of violence against children, again to promote standardised data collection and enable countries to produce comparable data.25 The International Classification on Violence Against Children underwent extensive consultation and testing. It was endorsed by the United Nations Statistical Commission in March 2023 as an international statistical standard and included in the family of official statistical classifications.25
This protocol outlines the plan for an international collaborative study aiming to build consensus on multi-sectoral definitions of CM, to address gaps or inconsistencies in the work outlined earlier.
Methods and analysis
Context and preparatory work
COST (European Cooperation in Science and Technology) is a funding organisation for research networks, and a COST Action is an interdisciplinary network that brings researchers together to investigate a topic of their choice. Euro-CAN (Multi-Sectoral Responses to Child Abuse and Neglect in Europe) is a COST Action-funded (CA19106) multi-disciplinary network of researchers and child protection practitioners from 34 countries in Europe and surrounding regions that provide unique perspectives on CM (www.cost.eu/actions/CA19106/). The network has established working groups to develop and promote a unified system of CM data collection in these countries. There are five working groups within the network, with Working Group 1 focused on initiating international, consensus-based, multi-sectoral processes for developing uniform classifications and definitions that can be used for CM data collection and surveillance in Europe.
Within Working Group 1, three pieces of preparatory background work have been conducted to investigate the topic from research, practice and policy perspectives and inform the development of this study. The first was a scoping review to identify the current gaps, key issues, challenges and debates in the literature about the definition and operationalisation of CM.26 A systematic search of eight international databases identified 25 recent studies (2011–2021) that satisfied the inclusion criteria. Only four studies reported attempts to create new conceptualisations or definitions of CM, and only one study tested their new definition in practice. The results indicated that more attention should be paid to the conceptualisation of psychological/emotional maltreatment and neglect during efforts to define and conceptualise CM. Finally, the importance of including child and victim perspectives on definitions of CM has started to be recognised in the literature.
The second was a comparative analysis of classifications and definitions of CM used by international organisations, which aimed to identify discrepancies between them and highlight key issues requiring consideration. We compared six classification systems, including the Modified Maltreatment Classification System,11 the Diagnostic and Statistical Manual of Mental Disorders, fifth edition and the International Classification of Diseases 11th Edition coding manuals,12 and classifications used by the following international organisations: the Centre for Disease Control10; the WHO and International Society for the Prevention of Child Abuse and Neglect14 15; and UNICEF.13 This analysis revealed that there is limited consensus on the types and subtypes of CM, or their definitions, between different classification systems. For example, consistent with the results of the scoping review, the analysis demonstrated that ‘emotional maltreatment’ is sometimes split into subtypes of ‘emotional abuse’ and ‘emotional neglect’ and sometimes considered as a single type of CM. In addition, the terms ‘emotional’ and ‘psychological’ are frequently used interchangeably.
The third was a survey of experts in CM (including paediatricians, social workers, lawyers and psychologists) to understand the similarities and differences in operational and legal definitions currently in use in child protection services and other public systems in the 34 Euro-CAN countries. This work showed substantial variability in the national operationalisations of CM for data collection purposes in different public systems, and revealed that Euro-CAN countries differ on whether and how CM is defined in legal documents.
Taken together, these results showed that the challenges regarding the definitions of CM are pervasive and continue to have implications for research, policy and practice. This background work was synthesised and discussed at a Working Group 1 meeting in October 2022, during which the key areas where consensus was lacking were identified, and the aims and objectives of this study were agreed. The study start date was 2 January 2023, with the protocol for the study agreed at a study steering group meeting at the end of January 2023.
Aim and objectives
The overall aim of this study is to reach consensus on operational definitions and types of CM for use in surveillance and multi-sectoral research in the 34 Euro-CAN countries.
The specific objectives are:
To develop consensus on the characteristics that distinguish ‘CM’ as a subset of ‘violence against children’.
To develop consensus on types and subtypes of CM.
To develop consensus on the minimum characteristics required to define an incident as CM, by type, for surveillance and research purposes.
Study design
This is an electronic Delphi study (e-Delphi). The Delphi method is a widely accepted, structured and systematic approach of gaining consensus on a particular topic through iterative rounds of anonymous responses from an expert panel.27 Panellists receive summary feedback on the group responses after each round. The method is increasingly used in health and social care research for a range of purposes.28–35 It has been used to build consensus on definitions,30 and has been demonstrated to be a valuable tool in multi-sectoral child welfare research.36 The methods in this paper are reported in accordance with suggested guidance for describing Delphi studies.37
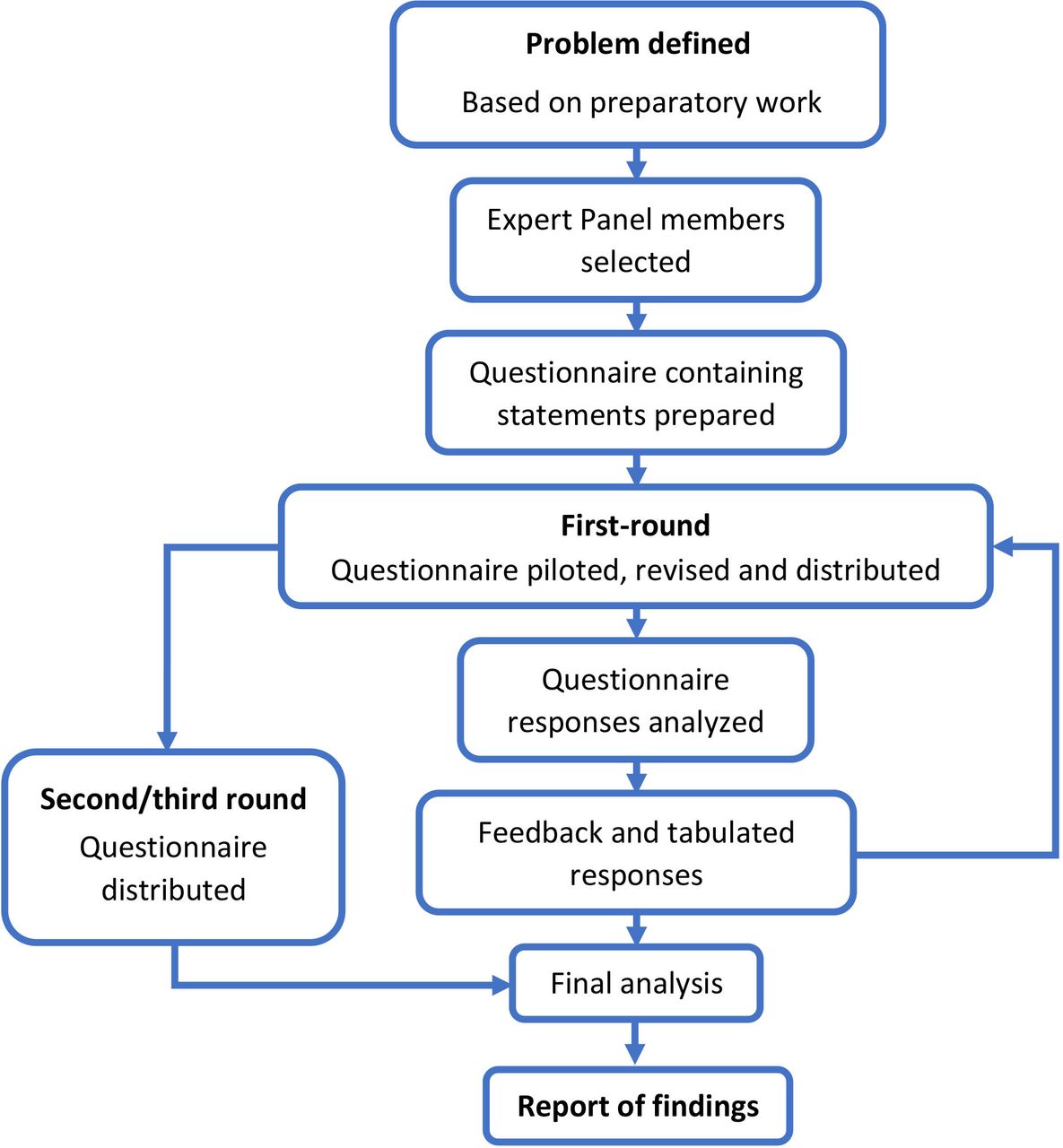
The e-Delphi process in our study will consist of a maximum of three rounds (see figure 1), with online data collection allowing experts from all 34 Euro-CAN countries to contribute. The questionnaire will initially include 13 statements relating to operational definitions and types of CM, based on the results of the preparatory background work. In round 1, participants will be asked to rate their agreement with the statements. Participants will also be asked to provide comments on each statement, to explain their responses and any areas of uncertainty. These comments will be used to refine the statements between rounds if no consensus is demonstrated. Comments will be analysed thematically by five members of the study steering group with experience of qualitative research (LEC, UN, KD, DL, LH), including three individuals whose first language is not English (UN, KD, DL). Participants will be asked to indicate where the wording of a statement is unclear or non-specific. Where multiple individuals indicate that this is the case, the wording will be discussed and clarified by the analysis team. Potential solutions will be presented to the wider steering group and a decision on wording changes made by consensus. Where there are indications that there is a genuine lack of consensus, reasons for this will be organised into themes. We will then either make changes to the wording of the statements and/or introduce new statements to explore these concepts further. These will be agreed with the steering group as above. Themes will not necessarily need to come from more than one expert type. However, as is standard in qualitative analyses, a theme will be generated if the opinion is expressed consistently across multiple participants.

{kind=link}
Flow chart for e-Delphi study.
In subsequent rounds, for statements that have not changed, participants will be asked to rate these statements again to examine the stability of agreement between rounds. For statements that have changed, participants will be shown the previous and adapted statements but will only be asked to rate the adapted statements. The total number of rounds (up to a maximum of three) will depend on consensus rates. That is, if consensus is reached for all statements after round 2, a further round will not be needed.
Recruitment of the expert panel
An international multi-disciplinary expert panel, who are independent of the study steering group, will be purposefully selected. This will consist of child protection professionals from health and social care, researchers, police and legal professionals, sociologists and individuals involved in policy development from the 34 Euro-CAN countries. Different eligibility criteria for each of the professions have been agreed by the study steering group (see table 1). In summary, the key characteristics for recruitment are significant practical experience and/or a robust research track record in CM, and the ability to understand the consent information and respond to the questionnaires in English. The experts will be identified from publications, internet searches and from the networks of the Euro-CAN members in the 34 countries.
Eligibility criteria for expert consensus panel
There are no formal sample size calculations in existence for Delphi studies. We are therefore taking a pragmatic approach, with the emphasis on recruiting experts with the right skills and knowledge and on maintaining a high response rate throughout the rounds. In this study, we will seek to ensure representation from a range of different disciplines, and at least one representative from each of the 34 Euro-CAN countries. Information on country and job role will be collected on the first questionnaire. This will allow the characteristics of contributing participants to be monitored as recruitment proceeds, with additional targeted approaches made to experts from under-represented countries or groups if needed. We anticipate approaching approximately 100 experts, and anticipate that 50–60 of these will agree to participate.
Potential participants will be approached via email by the study coordinator (UN). The invitation will include information about the study in an electronic participant information leaflet and a consent form which must be signed before they will be sent the link to the questionnaire. Participants will be advised to read the information leaflet and instructed to contact the study co-ordinator if they have any questions.
Development of the questionnaire
A steering group, consisting of members of Working Group 1 of the COST Action project (the authors of this paper), was convened to oversee the design of the study and data collection tools. This group developed the e-Delphi questionnaire by formulating statements relating to operational definitions and types of CM in areas that currently lack consensus. The initial questionnaire is divided into three sections to correspond with the three study objectives. It includes 13 statements in English, and participants will be asked to rank their agreement with these using a 4-point Likert scale (‘strongly agree’, ‘agree’, ‘disagree’, ‘strongly disagree’).30 38 There are also 21 open questions for participants to elaborate on their answers and/or make suggestions for additions or changes that can be incorporated into the statements for the next round. The questionnaire has been piloted with 12 members of the Euro-CAN network, to ensure clarity of language and format.
Patient and public involvement
We are working with Children’s Social Care Research and Development Centre (CASCADE) Voices (a care-experienced young people’s research advisory group) and the CASCADE Parents Research Advisory Group at Cardiff University’s School of Social Sciences to understand the perspectives of CM survivors and incorporate these into the work. Given the sensitive nature of the questions, it has been important to work with a well-established public involvement group with robust working methods and support mechanisms. The manager of the network (RV) has reviewed the protocol and questionnaire, and members of the group will be approached to participate in the expert panel. Although this is different from usual models of public involvement (where the public and patient representatives inform the design of a study), after discussion with network members and given the nature of this work, this was felt to be the most meaningful contribution that the group could make to the work. That is, they are experts because of their lived experience and therefore their perspectives should be included in consensus development. They will be supported to contribute to the expert panel by the manager of the network, and will be compensated for their time in accordance with the UK standards for public involvement in research.
Data collection
Data collection will take place between April and December 2023 (round 1 in April to June, round 2 in July to September, round 3 in October to December). We will use the online KoBo toolbox platform for data collection (https://kobo.humanitarianresponse.info). When the members of the international panel have returned their consent forms, a link to the first questionnaire will be shared with them. To ensure data completeness and improve the response rate, three reminder emails will be sent at each stage (recruitment, and each of the e-Delphi rounds). Once a participant has responded, they will be removed from the reminder list.
Data analysis
Response rates for each round will be collated and reported, along with the distribution of the individuals responding by expert type and country.
After the first round, we will calculate the percentage consensus for each statement based on the Likert-scale responses. A priori, we have defined consensus (ie, the extent to which the experts share the same view) as 70% or more of the panel members rating a statement as ‘agree’ or ‘strongly agree’, or 70% or more of the panel members rating a statement as ‘disagree’ or ‘strongly disagree’.30 39–41 If sample size allows, we will also examine agreement by professional group.
The responses to the open-ended questions will be analysed using an inductive ‘codebook’ approach to thematic analysis.42 43 Thematic analysis is a method for identifying and describing patterns across data, and such an approach is ideally suited to investigating professionals’ experiences and perspectives.44 45 The results will be reviewed by the steering group and used to guide discussions on changes to the statements or explanatory text where consensus has not been reached.
Agreement with both the unchanged and adapted statements will be examined in subsequent rounds. Participants will be provided with feedback and anonymised aggregate data at the start of the next round, to explain why and how the statements have changed. The same method of quantitative and qualitative analysis will be used to assess consensus after the subsequent rounds, with statements or explanatory text being adapted between rounds once results have been reviewed by the study steering group.
Statements achieving consensus after the final round will be used to identify operational definitions for research and surveillance. The stability of agreement will be assessed for all statements by examining the consistency of responses between rounds. After the final round, the results of the thematic analysis will be used to highlight any remaining differences in opinions and identify areas for future research.
Data analysis will be conducted in January and February 2024, with an anticipated end date for the study of 29 February 2024. The study results will be submitted for publication in a peer-reviewed journal by 1 July 2024.
Ethics and dissemination
Ethical issues
Ethical approval for the study has been granted by the Cardiff University School of Medicine ethics committee (reference number: SMREC22/96). The study will be conducted in accordance with relevant Cardiff University guidelines and regulations (including the Research Integrity and Governance Code of Practice and regulations governing research records retention and data protection).
The main ethical concerns relate to recruitment and participation; anonymity of participant information; appropriate storage of participant data which will comply with the General Data Protection Regulation and ensure data confidentiality; and the protection of the CM survivor participants as discussed below.
All potential expert participants will give informed consent to take part in the study. As all participants will be adults, they will be able to provide this consent themselves. They will be given the information leaflet and consent form prior to being recruited. The participant information will include detailed descriptions of the expectations of participation, including an assessment of the time it will take to complete the e-Delphi questionnaires. They will be informed that they do not have to answer every question, and that they can withdraw from participating at any time. Potential participants will be given an opportunity to ask questions about the study by email. Reminders will be sent on a weekly basis to allow the participants enough time to decide whether they wish to take part. Potential participants who respond by email to say that they do not wish to take part will be removed from the reminder list. The signed consent form must be returned to the study coordinator before the participant will be sent the survey link.
The anonymity of participants is an important ethical consideration in the Delphi method as the protection of anonymity ensures that experts can give their honest views. It also reduces any dominance of expert opinion between panel members and thus mitigates the risk of bias due to peer pressure within the group. Only one member of the study team will have access to information about the expert panel participants. Any responses made available to other participants or in any study publications or presentations will either be in aggregate form or fully anonymised.
The main risk to confidentiality and security of information is data breaches. Participants’ names, email addresses and roles will be requested at the time of enrolment, prior to round 1. Only one member of the study team will have access to this information. A split-file data storage system will be used where this identifiable information and the questionnaire data will be stored in separate databases, linked using a unique participant identification number. Data will be stored electronically on Cardiff University servers, which are backed up daily. To further mitigate against data breaches, all project staff are trained in Information Security and Research Integrity and Governance principles.
Although the questionnaires will contain potentially distressing information on different types of CM, it is not anticipated that this will cause distress to the members of the expert panel who are child protection professionals, as this information will not relate to specific cases of CM and will use language that these professionals use daily in their work. It is, however, important to consider the potential impact of these statements on the CM survivors who will be recruited as part of the expert panel. We chose to work with CASCADE public involvement groups to identify suitable individuals to take part in the study because they are well-established public involvement group with robust working methods and support mechanisms. Therefore, CM survivors involved in CASCADE public involvement groups have elected to take part in supporting research projects. Detailed information will be provided to the individuals who take part in the study in advance of their participation, to prepare them for the questions. The Engagement Manager at CASCADE will also work with the survivors as they complete the questionnaires, to provide support in case of the need for clarification or emotional support.
Dissemination
Results will be reported in accordance with the CREDES Guidance.37 In addition to the consensus results, we will describe the response rates and changes in response rates between rounds, as well as any modifications of the survey instrument such as deletion, addition or modification of survey items between rounds.
At the end of the e-Delphi study, we will arrange a workshop with all participants to present the results to them. This workshop is for dissemination only, and no additional data will be collected at this time. The results will be submitted for publication in a peer-reviewed journal(s) and for presentation at international academic conferences. The networks of Working Group 1 members will be used to disseminate the results in the 34 Euro-CAN countries, with results briefings and presentations offered to key public health and other relevant organisations in the field.
The datasets generated and/or analysed during the current study will not be publicly available due to the sensitive nature of the study subject matter and the potentially identifiable nature of the data (due to the information that will be collected on country of residence, profession and qualitative data, especially in combination), but may be available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Ethics Committee of Cardiff University School of Medicine (SMREC22/96, date of initial approval 20th December 2022; approval of subsequent amendments 23rd February 2023).
References
Footnotes
Twitter @LauraCowley28, @lisashurt
Contributors UN, LEC, LBR, AN, GD, RA, DL, GO, AJ, AN, TL, VSoldino, VStancheva, LC, RV, CWC, KD, AMK and LH contributed to the conceptualisation and methodology of the study. LH, LEC, UN, AN, GD and RA contributed to the writing. UN, LEC, LBR, AN, GD, RA, DL, GO, AJ, AN, TL, VSoldino, VStancheva, LC, RV, CWC, KD, AMK and LH contributed to reviewing and editing. All authors have read and agreed to the published version of the manuscript.
Funding The work is funded by Public Health Wales (grant reference: National Safeguarding Delphi Project). One of the author’s (AN) is an employee of Public Health Wales, in her role as Service Lead for the National Safeguarding Team (NHS Wales). No other member of Public Health Wales staff had a role in the design of the study, and collection, analysis and interpretation of data and in writing the manuscript. The work developed by ProChild CoLAB (co-author LBR) was supported by FCT – Fundação para a Ciência e Tecnologia, I.P. - and NORTE-06-3559-FSE-000044, integrated in the invitation NORTE-59-2018- 41, co-financed by the Regional Operational Programme of the North 2020, thematic area of Competitiveness and Employment, through the European Social Fund (ESF).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.