Article Text

Abstract
Objectives To investigate the effect of age-related rotator cuff tears on shoulder strength in a general population cohort.
Design Cross sectional observational study.
Setting This study was set in an outpatient clinic setting in Chingford, North East London, and was a component of the 20 year visit of the Chingford 1000 women cohort.
Participants Individuals were part of the Chingford 1000 women cohort, a 20-year-old longitudinal population study. This cohort has been extensively characterised as representative of the population of the UK. At the 20 year visit, 446 attended for shoulder assessment and were aged between 64 and 87.
Primary and secondary outcome measures Isometric shoulder abduction strength measured using a Nottingham Mecmesin Myometer and the presence of rotator cuff pathology, determined via ultrasound examination (GE voluson i portable ultrasound machine with a 10-16MHz linear probe). Shoulders were classified into normal, abnormal tendon/partial tear, full-thickness tears (>0 and ≤2.5 cm) and full-thickness tears (>2.5 cm). Symptoms were defined using the Oxford Shoulder Score, where an abnormal score was defined as symptomatic.
Results 446 women (891 shoulders) aged 71 (range 65–84) were included in the study. Age, the presence of pain and the non-dominant arm were demonstrated to reduce strength. Rotator cuff tears and pathology had no isolated effect on shoulder strength in those aged under 70. However, in the over 70s full-thickness tears>0 and ≤2.5 cm, and >2.5 cm had mean reductions of 6.3 and 12.7 N, respectively (p<0.001).
Conclusion Rotator cuff tears of all sizes in those aged under 70 were not associated with a loss of shoulder strength. In those aged over 70, strength was reduced by 30% with small and 40% with large full thickness tears. Loss in strength was associated a loss of ability to perform activities of daily living but only for large tears.
- Shoulder
- Musculoskeletal disorders
- Adult orthopaedics
Data availability statement
Data are available upon reasonable request. Deidentified data are available on reasonable request. Information regarding the Chingford 1000 Women Study data can be found at: https://www.hra.nhs.uk/planning-and-improving-research/application-summaries/research-summaries/chingford-1000-women-study/. Enquires can be made to: Nigel.Arden@ndorms.ox.ac.uk.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Population-based study: participants are from an established population cohort, that has been extensively described in the literature as representative of the general population of the UK.
The cohort includes the age of interest in this study of the >60s, although women only.
Observer and analytic bias: the study was performed by a single observer—multiple blinded observers were limited by resources.
Assessment of global shoulder strength was measured using two functional positions in the sagittal and coronal planes—strength measurements were not performed in the transverse plane.
Introduction
Background
Musculoskeletal shoulder pain and dysfunction prevalence in the community is historically reported to be 20%.1 Full thickness tears are present in greater than 20% of the population aged over 60, and cause pain in 32% of these.2 It is purposed that functional deficits of the shoulder may be due to strength loss with or without the presence of pain, however causation has not been determined.
Shoulder strength can be measured quantitatively, using hand-held,3 isokinetic or externally fixed dynamometry4 or myometery, and is a key component of commonly used patient reported outcome measures, including the Constant score5–11 and the American Shoulder and Elbow Surgeons Score (ASES).12 These provide information on shoulder pain and function, are used clinically by Orthopaedic surgeons to detect response to treatment, and by general practitioners as cost-effective screening tools to direct medical management.9 13
Normative values for shoulder strength stratified for biological sex and age deciles have been established, and found to significantly decrease with increasing age14 and female gender.9 Though, the relationship between rotator cuff tears and strength in asymptomatic shoulders is not clear.14 15 The shoulder function of people with symptomatic and asymptomatic rotator cuff tears on activities of daily living has been studied in a rural Japanese mountain population.16 This study did not assess shoulder strength functionally, and instead used the Simple Shoulder Test (SST).17 It reported that participants with a rotator cuff tear, including those without pain, reportedly were less able to lift a 3.6 kg weight to shoulder level. A longitudinal cohort (Rotator Cuff Outcomes Workgroup: ROW) study investigating a group of individuals with shoulder pain found decreased shoulder abduction and external rotation strength in those with a supraspinatus tear on MRI.18 However, no study to date has measured shoulder strength in association with rotator cuff tear in a general population cohort. This information will improve the understanding of rotator cuff tear and its relationship to shoulder strength and symptoms.
Objectives
The primary objective of this study was to establish the effects of rotator cuff tear on shoulder abduction strength using a hand-held dynamometer, a clinical and pragmatic measurement tool. Our secondary objectives were to determine the potential interaction effect of age on shoulder abduction strength, and if a correlation exists between shoulder abduction strength and self-reported shoulder function using the Oxford shoulder score.
Methods
Study design, setting and participants (including study size)
Participants involved in a large prospective population-based longitudinal study of osteoarthritis and osteoporosis (Chingford Study North London19–21) were invited to complete a shoulder examination. The Chingford study comprised initially of 1003 white Caucasian women aged 44–67 years at baseline that have been extensively characterised as representative of women in the UK general population with respect to weight, height and smoking characteristics.20 It has been listed by the National Institutes of Health as an important epidemiological resource collecting musculoskeletal data. This study took place at the 20 year follow-up of the Chingford cohort; 516 women remained in the cohort and attended this follow-up. Of the 516 women, 446 women agreed to complete a bilateral shoulder assessment inclusive of musculoskeletal examination, strength test, ultrasound and series of questionnaires (Oxford Shoulder Score,22 23 body chart and general questions about previous pain, treatments and whether medical advice has been sought). These women were characterised as representative of the original cohort, and at the time of data collection were aged between 64 and 83.
The ultrasound examination was performed using by an orthopaedic surgeon, using an imaging protocol recommended by the Nuffield Orthopaedic Centre Musculoskeletal radiology department. Tendons were categorised using a validated classification system: normal tendon; abnormal tendon and partial thickness tear; single tendon full-thickness tears (>0 and ≤2.5 cm) and multitendon full-thickness tears (>2.5 cm).24 Results of the ultrasound examination in this cohort have been previously published.2
Pain was defined for each shoulder using the OSS. Any abnormal score in the four pain questions was defined as symptomatic. Justification for this use of the score is described in our previous study.2
Consent was obtained from each participant and the Outer North-East London Research Ethics Committee (formerly Barking and Havering and Waltham Forest RECs) approved the study, reference LREC (R&WF) 96.
Variables and data sources
Outcome measures
Participant characteristics including age, height, weight and hand dominance were filled out a priori. The presence of shoulder symptoms was measured using the Oxford Shoulder Score,23 25 a validated self-administered questionnaire. Pain was defined as any abnormal result in one or more of four pain specific questions. Function scores were defined using the eight function-based questions of the score as a total out of 32 points.
Isometric shoulder strength was measured using the Nottingham Mecmesin Myometer (Mecmesin Ltd, UK). Strength was assessed according to recommendations by the European Society of Shoulder and Elbow Surgery (www.secec.org), and is the same technique as described by Constant et al,5 6 standardised by Bankes et al7 in obtaining the Constant shoulder score. The participant was seated with the hips at 90° flexion and both feet flat on the floor. Shoulder abduction strength was tested with the arm at 90° in the plane of the scapula (30° forward in the coronal plane), with the elbow straight and the palm facing the floor. Flexion strength was tested with the arm at 90° in the sagittal plane, again with the elbow straight and the palm facing the floor. The individual maintained resisted elevation for 5 s, and the maximum strength recorded. This was repeated three times, and the mean maximum strength was recorded for each arm.
Quantitative variables and statistical methods
All statistics were performed using IBM SPSS Statistics V.22 (IBM, Armonk, New York, USA). Age, body mass index (BMI), arm dominance and symptom presence were compared across the four tendinopathy groups. Wilcoxon rank sum test, one-way analysis of variance (ANOVA) and χ2 tests were used for non-normal, normal and categorical data, respectively.
Shoulder abduction and flexion strengths were compared across each tendinopathy group using a one-way ANOVA. A univariable linear regression model was performed to determine the effect of rotator cuff pathology on strength. Univariate and multivariable regression models were used to identify confounding and interacting variables. A final multivariable linear regression model, with observed power of >0.8, followed with adjustment for potential confounders age, pain presence and hand dominance along with subsequent interactions. A Spearman’s rank correlation coefficient was used to determine association between the quantitative strength and the patient reported functional deficit.
Patient and public involvement
None
Results
Participants and descriptive data
There were 446 individuals (891 shoulders) included in the study. Age was not normally distributed, and the median age was 71 (range 65–84). BMI was normally distributed with a mean of 27.8.
Baseline demographics including age, height in centimetre (wall-mounted stadiometer) and weight in kilogram (electronic scales and shoes removed), presence of shoulder symptoms (Oxford Shoulder Score23 25 and tendon pathology classification24) of the 891 shoulders are shown in tables 1 and 2.
Baseline demographics for each shoulder, and the prevalence of tendinopathy according to age decile
The prevalence of all shoulder tendinopathy according to age decile
Age was statistically different between groups (Kruskal Wallis Test, p<0.001). There was no statistical difference in BMI (mean 27.8) between groups (one way ANOVA, p=0.078). There was no difference in right-hand or left-hand dominant individuals in each tendon pathology group (χ2, p=0.807), however there was a statistical difference in dominant and non-dominant arms between groups (χ2, p=0.047).
The number with pain varied between groups: of the normal tendons, 82 (16.8%) had; for abnormal/partial tears (31.3%); for full-thickness tears>0 and ≤2.5 cm (34.6%); for full-thickness tears>2.5 cm, 25 (67.6%) had pain, respectively. This was statistically significant between groups (χ2 linear association, p<0.001).
Outcome data and main results
Quantitative strength assessment
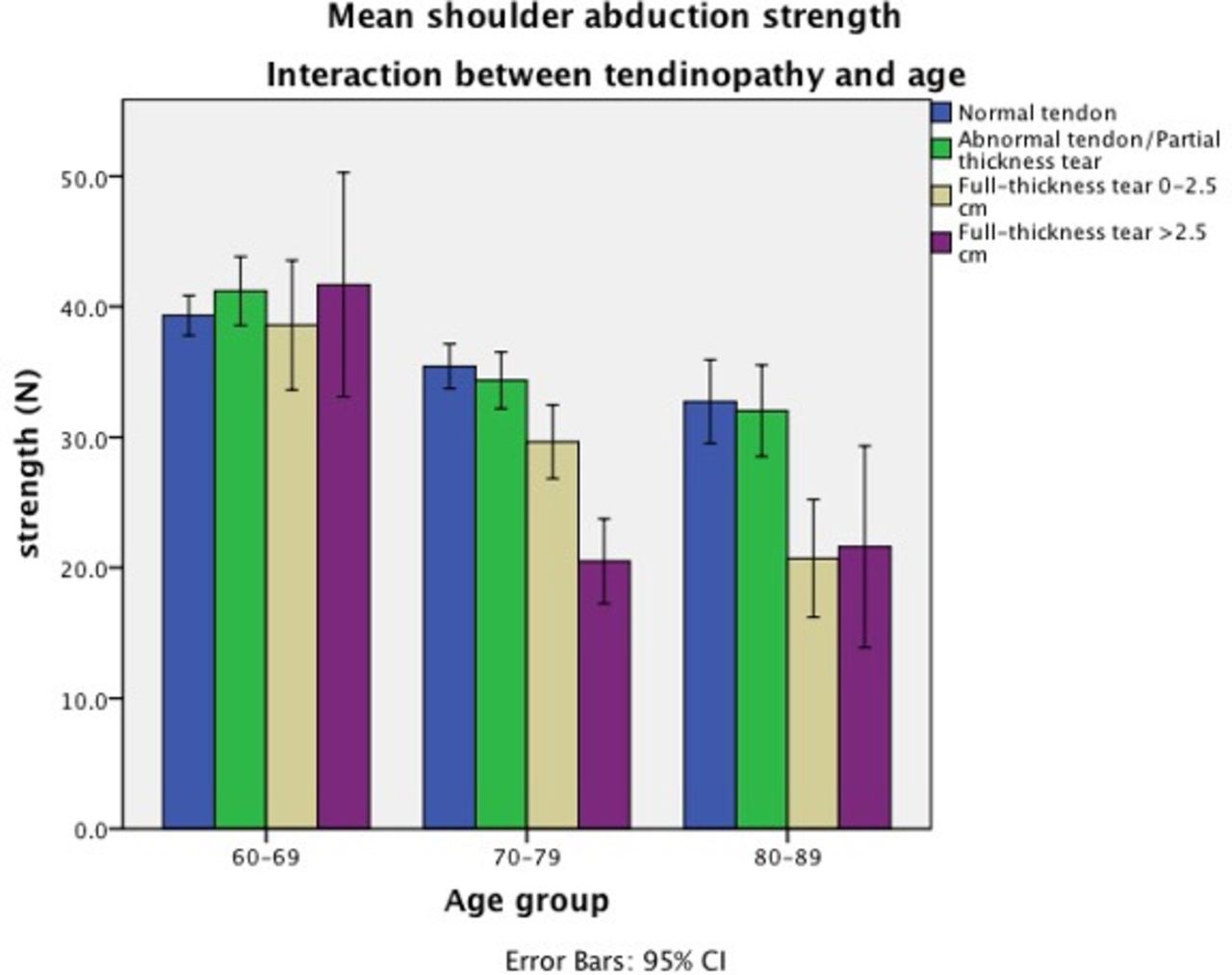
Shoulder abduction strength was normally distributed. Mean shoulder abduction strength was 35.5N. For normal tendons, this was 42.0N (95% CI: 35.7 to 37.0), abnormal/partial tears 39.8N (95% CI: 34.8 to 37.9), full-thickness tears>0 and ≤2.5 cm 33.4N (95% CI: 27.9 to 32.9) and full-thickness tears>2.5 cm 24.1N (95% CI: 20.5 to 27.8). The difference between groups was clinically significant (one-way ANOVA, p<0.001). Linear regression demonstrated there to be no significant difference between normal tendons and the abnormal tendon and partial thickness tear group. However, there were mean reductions compared with normal tendons of 6.3N and 12.7N for the full-thickness tear>0 and ≤2.5 cm and >2.5 cm groups, respectively (p<0.001). The presence of pain, and hand dominance was shown to have a confounding effect on shoulder strength across all groups. Age showed interaction effects on strength as tear stage severity increased.
A multivariate regression analysis was performed to show the relationship between shoulder abduction strength and tendinopathy, age, hand dominance and pain. The mean dominant arm abduction strength (N) for an individual aged 60–69 with an asymptomatic shoulder and normal ultrasound was 41.4N (p<0.001, power 1.0). Pain confounded with a 10.8% (4.5N) mean reduction in strength (p<0.001, power 0.96). Non-dominant arms confounded with a 4.9% (2.03N) reduction in strength (p=0.011, power 0.72). Overall, the 70–79 age group with normal tendons had a reduction in strength of 10.2% (4.2N) (p<0.001, power 0.96), and the 80–89 age group 16.2% (p<0.001, power 1.0). Tendon pathology classification group did not have an isolated effect but was found to interact with age. Such that there was no reduction in strength for the 60–69 group in the presence of tendon pathology, however for large tears in the 70–79 age group, strength was reduced by 39.0% (p=0.003, power 0.84), and the 80–89 age group, 30.2% for small tears (p=0.004, power 0.82), and 32.2% for large tears (p=0.050, power 0.49) (figure 1).

The impact of tendon classification and age on shoulder abduction strength.
A weak-moderate correlation of 0.238 was found between the Oxford Shoulder score (function subset) and shoulder abduction strength in those with symptomatic full-thickness tears (n=53) (p<0.001) (figure 2). This suggests a poorer ability to perform activities of daily living in people with symptomatic cuff tears, that have less shoulder abduction strength.

{kind=link}
{kind=link}
Correlation between the Oxford Shoulder Score (OSS) function subset and shoulder abduction strength in symptomatic full thickness tears (FTTs).
Discussion
Key results
This population-based study has measured shoulder abduction strength quantitatively in a large general population cohort. It has shown that both small and large rotator cuff tears are associated with a loss of shoulder strength, but not in isolation. Shoulder strength was found to reduce with increasing age, the presence of pain and in the non-dominant arm. The presence of rotator cuff tear had no isolated effect on strength, however when interacting with age, a significant effect was present. Irrespective of the presence of any size rotator cuff tear, strength was preserved in those aged 60–69, however in those aged 70–89, there was a 33–39% decrease in strength in the presence of rotator cuff tear depending on the age of the individual and the size of the tear. With adjustments made for the increased prevalence of tears with age, this interaction could be representing a lack of ability to compensate for a rotator cuff tear in the older age groups.
Limitations (including bias)
The potential limitations of this study are observer bias and analytic bias. The study was performed by a single observer and followed a fixed order of data collection. This involved a subjective symptom assessment followed by strength assessment followed by an ultrasound examination. It is possible that symptom and strength assessment could have influenced the report of the ultrasound, which in turn could have strengthened any association and enhanced the confounding effect of pain. This was a pragmatic study, and resources limited the use of multiple blinded observers.
Although we have followed standardised recognised methods of strength assessment, it is difficult to ensure that all individuals perform the test in the designated manner. The method is based on isolating shoulder strength and relies on not using major core muscles. Though recruiting core muscles may have happened uniformly across all tendinopathy groups, it is possible that those with pain or weakness were more prone to adapting the technique to generate power. If this occurred, this would have lessened any association of strength between either pain or pathology.
In this study, we have collected data from both shoulders of the participants. These have been analysed as statistically as independent variables. It is acknowledged that overall data are not fully independent, however as the primary outcome is related to shoulder strength in relation to pathology, rather than symptoms, which are influenced by the individual, statistical differences in strength are not subject to this bias. Furthermore, given that all data, including strength and symptoms, were collected for each shoulder, and that symptom assessment was assessed only its confounding role, the potential bias of the individual in relation to symptoms is negligible.
Relationship to other studies
The cohort used in this study was established by invitation from a general practitioner registry, with the primary goal of investigating osteoporosis. It was not subject to attrition bias, or selection bias as it was not selective to those with shoulder problems. This was further strengthened by the lack of a known association between osteoporosis and rotator cuff tears. The study could have been affected by survivor bias, however results have been stratified by age to reduce this effect. The only selection bias for this study is that it includes only older women, and thus results are only generalisable to women aged 65–89 in the UK.
The current population-based study has looked at shoulder strength in relation to rotator cuff tears in both painful and pain free shoulders, and therefore is not subject to significant selection or estimator bias. To the authors knowledge, there is only one other population-based study of shoulder strength that has reported on manual muscle testing25 and the SST to define strength, in two studies from the same cohort.17 26 However, there are numerous published studies on shoulder strength in the presence of rotator cuff tear in smaller cohorts.14 18 27
Shoulder abduction strength is reported to be negatively impacted by the presence of rotator cuff tear in both symptomatic and asymptomatic populations. Miller et al18 investigated shoulder strength in a cohort of 208 people (male and female) aged>45 with shoulder pain. Shoulder abduction strength was lower in people with supraspinatus tear (3.9 kg) compared with those without a tear (5.3 kg) (p=0.02) when measured using hand-held dynamometry. Furthermore, age greater than 60 years, female sex and pain score on visual analogue scale were found to be associated with lower shoulder abduction strength. Consistent across the study by Miller et al,18 and the Chingford Cohort is the negative impact of increased age; presence of rotator cuff tear on declining shoulder abduction strength and the lack of an isolated effect of tendon pathology severity on shoulder abduction strength. Furthermore, a lack of association between tear severity and shoulder abduction strength has also been reported on 61 patients with symptomatic shoulders awaiting surgery (n=50 with rotator cuff pathology).27 No significant difference in shoulder abduction strength was measured at 90°, however it was significant at 10° in the scaption plane.
Kim et al14 investigated the rotator cuff of 237 individuals (n=93 female) with asymptomatic shoulders, using ultrasound, and reported an age-dependent decrease in shoulder abduction strength in female subjects with intact rotator cuff in both dominant (β=−0.401) and non-dominant arms (β=−0.411). The Chingford and Kim et al studies both used the Constant and Murley shoulder assessment protocol for shoulder abduction strength measurement. However Miller et al completed testing in 45° of horizontal flexion,18 and McCabe reported results with respect to the ‘scaption’ plane, and not a specific position using degrees.27 Heterogeneous methodology may account for differences in results noted between studies.
Dominant shoulders are reported to have greater strength compared with non-dominant shoulders in female subjects with asymptomatic shoulders and no tear.14 The Chingford cohort supports the results of this previous study. Non-dominant shoulder abduction strength (N) for an individual aged 60–69 with an asymptomatic shoulder and normal ultrasound was found to have 4.9% less strength than in dominant shoulders.
Interpretation
This general population cohort study provides a scholarly contribution to the literature available on rotator cuff tear, and the resultant impact on global shoulder strength (measured using the Oxford Shoulder Score). Size of tear in people under 70 years was not associated with a loss of shoulder strength. In those aged over 70, strength was reduced by 30% with small and 40% with large full thickness tears. Loss in strength was associated a loss of ability to perform activities of daily living but only for large tears. This may provide a window of opportunity for rehabilitation strength exercises to be implemented prior to 70 years—particularly in those with pathology in the non-dominant arm, to lessen the impacts of strength loss and associated functional impairment following this time. Though, further research would be required to test this assumption.
Generalisability
The results of this study are generalisable to the UK population and have possible application to white Caucasian women in developed countries, aged 65–89 years.
Conclusion
This study investigates shoulder abduction strength in association with rotator cuff tears in an established and extensively characterised general population cohort of women, and has demonstrated a novel interaction between age, rotator cuff tear and hand dominance that affects subsequent strength and the ability to perform activities of daily living.
Data availability statement
Data are available upon reasonable request. Deidentified data are available on reasonable request. Information regarding the Chingford 1000 Women Study data can be found at: https://www.hra.nhs.uk/planning-and-improving-research/application-summaries/research-summaries/chingford-1000-women-study/. Enquires can be made to: Nigel.Arden@ndorms.ox.ac.uk.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. Ethics approval: Outer North East London Research Ethics Committee (formerly Barking and Havering and Waltham Forest RECs), LREC (R&WF) reference ID = 96. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank all the participants of the Chingford Women Study for their time. We would also like to thank Mrs Maxine Daniels and Dr Alan Hakim for their time and dedication, and both Mr Alex Nichols and Mr Michael Daines for their assistance with data collection and Dr Gemma Wallis for reviewing statistical analysis processes used in this study.
References
Footnotes
NKA and AJC are joint senior authors.
Contributors HH, NKA and AJC were responsible for planning, conducting and reporting the work described in the article. HH and CG drafted the manuscript. All authors approved the final version of the article. HH, NKA and AJC had access to all the data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. HH is guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. All authors fully acknowledge the contribution of the patients who participated in this study. No authors are employees of the National Institutes of Health.
Funding Arthritis Research UK awarded the project £190 361.00 to cover costs to completion (ref number 19550). Researchers were independent from the funding body. All authors, external and internal, had full access to all the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.