Article Text

Abstract
Objectives Multimorbidity challenges healthcare systems. In Germany, coordination of healthcare for older multimorbid patients remains unstructured.
This study aims to identify key themes in the healthcare of these patients and the inter-relationships between them.
Design Framework analysis of six cases based on 1-year data of primary and secondary care, patient-answered questionnaires and video material.
Setting Southern Germany.
Participants Six multimorbid older patients participating in a randomised controlled trial that compared usual care with a local, collaborative, stepped and personalised care management approach for older people with chronic diseases (LoChro-trial). The LoChro care intervention involved a care manager who assisted participants in self-management. The primary outcome was a composite of functional health and depressive symptoms at 12 and 18 months. The LoChro-intervention had no effect on the primary outcome.
Primary outcome measure Key themes in the healthcare of older patients with multimorbidity and the inter-relationships between them.
Methods One-year data included diagnoses, treatment plans, examinations, assessments and discharge reports. Patient perspectives were assessed using the Patient Assessment of Chronic Illness Care. In three cases, videos of the LoChro intervention showed patients describing their health needs. These data were evaluated by three doctors and public health researchers. Using framework analysis, recurring themes influencing the healthcare situation of multimorbid older patients and their inter-relationships were identified.
Results Participants had an average age of 77, with 13 diagnoses, taking eight medications regularly. The five key themes describing the healthcare situation of these multimorbid patients were as follows: insufficient coordination, overuse and underuse of medical care, doctor and patient roles. Each theme covered three to four subcategories. The most significant inter-relationships between these themes were a lack of coordination leading to overuse and underuse of medical care. These were characterised by redundant inpatient stays, potential prescribing omissions and missed examinations. Deficiencies in vaccinations and secondary prevention were also demonstrated.
Conclusion Coordination of care for multimorbid older patients in Germany is still deficient. Future healthcare arrangements should be explored with the participation of physicians and patients.
Trial registration number LoChro trial: DRKS00013904.
- GENERAL MEDICINE (see Internal Medicine)
- PUBLIC HEALTH
- GERIATRIC MEDICINE
- Organisation of health services
Data availability statement
Data are available upon reasonable request. The data sets used and analysed during this study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- GENERAL MEDICINE (see Internal Medicine)
- PUBLIC HEALTH
- GERIATRIC MEDICINE
- Organisation of health services
STRENGTHS AND LIMITATIONS OF THIS STUDY
Identification of key themes in the healthcare of older patients with multimorbidity in Germany and the inter-relationship between themes, using framework analysis.
The direct link between real-life cases, including the perspectives of patients and public health aspects of care.
The evaluation of cases by general practitioners and public health researchers central to the interprofessional team of the LoChro trial.
Six case examples illustrating the healthcare experiences of older patients with multimorbidity in Germany.
The limited availability of data in primary care in Germany.
Background
Worldwide multimorbidity has become a major health problem. Multimorbidity is often defined as the co-occurrence of two or more physical and/or mental conditions.1 In the UK in 2015, 9.8% of the population were living with more than four chronic diseases and approximately 17% of the population is expected to face multimorbidity by 2035.2 The international median cumulative incidence of suffering with more than one chronic condition was estimated at 2.8% in a recent systematic review.3 For this reason, health policy makers and other stakeholders are increasingly seeking to adopt entire healthcare system strategies to combat multimorbidity,4 investigating patients with multimorbidity and their current healthcare needs in a more comprehensive manner.5
As in other nations, most patients visiting a general practitioner (GP) in Germany are generally older and multimorbid.6 7 Multimorbidity appears subject to an overuse of medical resources, as a recent investigation into the healthcare records of a German health insurance company revealed.8 However, multimorbidity, often prompting polypharmacy, may even be related to underuse of medical care.9–11 In this context, coordination and continuity of care gain crucial roles in optimising the care of patients with multimorbidity.12 13 On the one hand, continuity of care poses a challenge to established healthcare sectors,14while, on the other hand, it is associated with desirable outcomes; namely fewer hospital admissions for conditions that are amenable to management in the ambulatory care sector15 with corresponding reductions in mortality.16
The German healthcare system is mostly publicly organised; employers and employees finance the public health sector equally. In addition, private care suppliers and private insurance companies exist. There is a strong separation of the outpatient and inpatient sectors, with interface problems often being exacerbated by delayed digitalisation.17 18 In the German healthcare system shaped by federalism, there are no formal structured health arrangements for multimorbid patients.
Policy makers, however, acknowledge the challenge that primary care is facing especially on the background of scarce human resources.19 Hence, as seen in other countries, several efforts to strengthen integrated care for people with multimorbidity have been made, including the implementation of the Primary Care Practice-Based Care Management model in southern Germany and GP-centred-care (Hausarztzentrierte Versorgung).20 21 Although both programmes show promising results regarding decreasing numbers of hospitalisations, cost and high patient satisfaction,22–24 up to now only a few patients appear to be enjoying these benefits. Only 6% of the German population participate in GP-centred-care.25 26
Interviews with health professionals, including doctors and healthcare assistants, as well as interviews with patients, has brought insights into their personal experiences with multimorbidity.27 28 In a qualitative analysis of interviews with GPs and their corresponding multimorbid older patients, GPs focused more on potentially life-threatening events, while patients put more emphasis on autonomy and social participation.28 In addition, GPs felt poorly informed about local schemes for multimorbid patients, seeking greater support in referring their patients to social services.29
A systematic guideline review identified not less than 10 guidelines on multimorbidity or polypharmacy, that intended ‘to make explicit recommendations with a definite intent to influence what clinicians do’, two of them published in Germany.30–32 The reviewers grouped the 246 recommendations from these guidelines into the following areas: identification of the target population, interaction assessment, patient preference, prioritisation and goal setting, individualised management and monitoring and follow-up. These were mainly based on the Ariadne principles of counselling for patients with multimorbidity.30 33 In addition, it was advised that clinicians dealing with older multimorbid patients should follow the vaccine recommendations of the national vaccine committee,34 guidelines for geriatric assessments in primary care,35 national and international disease-specific guidelines and may use, eventually, IT systems that can detect potentially inappropriate medications (PIM) and potential prescribing omissions (PPO).36–38
This study is based on a detailed 1-year analysis of the care situation of six multimorbid older patients participating in a randomised effectiveness trial that compared the effects of a local, collaborative, stepped and personalised care management approach (LoChor care) for older people with chronic diseases with usual care (LoChro trial).39 Participants of the intervention group received between seven and 13 contacts with specifically trained care managers who supported participants in self-managing their care. During the intervention, patients were prioritised based on their health issues. However, these care managers had no contact with other caregivers, such as GPs. The LoChro trial was completed in 2022. Neither effects of LoChro care on the primary outcome, a composite of functional health and depressive symptoms, nor the secondary outcomes, which included the evaluation of their health situation by participants, health-related quality of life (HRQoL) and life satisfaction, could be detected.40 The objective of this investigation was to highlight any recurring themes gleaned from the healthcare situation of multimorbid older patients in southern Germany, and to highlight the inter-relationships of these themes. As such, these healthcare situations encompass diagnostic processes, the prevention and treatment of physical and mental health conditions and the use-pattern of the health service by multimorbid older patients. The overarching aim of this qualitative analysis was to present insights into the current healthcare situation of multimorbid older patients and to help identify potential targets for optimisation, such as hidden health service gaps, communication errors or incentive problems, as prerequisites for further intervention trials.
Methods
Study population
The LoChro trial recruited patients who were aged 65 or more, and were at risk of loss of independence, measured using the Identification of Seniors at Risk Screening (ISAR) Tool41 in the inpatient and outpatient departments of the local university hospital. The ISAR, a six-item score, has been shown to be associated with unplanned readmissions, institutionalisation and the need for nursing care in older patients in Germany.42 Exclusion criteria for the LoChro trial were as follows:1 terminal medical conditions,2 lack of basic German-language skills or no German-speaking caregiver available and3 not residing in the region.39
Choice of six participants for this study
The grant application for the LoChro trial submitted for approval to the German Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung, BMBF) already outlined this investigation. Due to the finite resources available at the time and the detailed, in-depth focus of this investigation, a maximum of six subjects were recruited. Initially, 2721 people took part in the eligibility assessment of the LoChro trial, 524 participated in the trial, 261 were allocated to the intervention and 263 to the control group; 81 were lost to follow-up 1 year after recruitment (t1) in the intervention group and 79 in the control group. Out of all the patients still taking part in the LoChro trial 1 year after recruitment, six participants were chosen for the more detailed analysis of their healthcare situation in the preceding 12 months. Half of these participants received the LoChro intervention which comprised the engagement of trial-specific care managers having regular contacts with the patients to support self-management.39 The other three participants received the usual care. The three participants of the LoChro intervention group were chosen randomly. Three control group participants were matched at baseline according to the variables age, sex, score of the WHO Disability schedule 2.0 (WHODAS), measuring functional disability43 and Patient Health Questionnaire Score-Depression (PHQ-D).44 These six individuals constituted the study population for this investigation. The study assessors remained blinded towards the LoChro group-variable until an initial evaluation of the healthcare situation of all six participants was agreed on. Later in the process, they were un-blinded for these six patients, to integrate the video material of the intervention into their evaluation.
Data source
The aim of this study was to obtain a complete picture of patient health contacts over the course of a year. For triangulation purposes, three main sources provided the data for this research: the local university hospital records, outpatient carers, and the patient’s own perspective.
First, the investigators had access to the documentation system of the local university hospital, where all participants had been treated. Specifically, the authors could study discharge letters, diagnostic results, including radiological, laboratory and other results, hospital inpatient medication lists, consultation and conference reports.
Second, on at least two occasions, outpatient carers of the six patients were asked openly to deliver as much information on outpatient care over the last 12 months as possible, including medication and treatment plans, specialist reports, clinical, including geriatric assessments, laboratory examinations and other documentation.
Third, the patient perspective was included in the analysis as the investigators had access to the responses of the participants to the following questionnaires used in the LoChro trial at baseline and 1-year follow-up:
The WHODAS 2.0 measuring functional disability.43
PHQ-D.44
A German questionnaire assessing the healthcare services used by older patients: Fragebogen zur Erhebung von Gesundheitsleistungen im Alter (FIMA).45
Patient Assessment of Chronic Illness Care (PACIC)46 measuring patient satisfaction with their healthcare (see below).
A questionnaire on diagnoses and medications that were, possibly, not documented by clinicians (such as constipation or the regular intake of calcium and vitamin D supplementation) but relevant for the Screening Tool of Older People’s Prescriptions and the Screening Tool to Alert to Right Treatment (STOPP/START V.2) used for assessing potentially inadequate medications (PIM) and PPO.36
A one-item scale on HRQoL (How would you rate your health status in the last 3 months on a scale from zero to 10, zero meaning very poor and 10 meaning excellent?’)
A one-item scale on life satisfaction.47
Patient Assessment of Chronic Illness Care (PACIC)
The PACIC is of a special relevance to this study as it measures patient satisfaction with healthcare exposure. It was validated for use in patients with chronic diseases in Germany and consists of 12 domains46 on a 10-step Likert scale from 0% to 100%, where 0% represents ‘true for none of my doctor’s consultations in the last 6 months’ and 100% indicates ‘true for all of my doctor’s consultations in the last 6 months’.
In the three cases that received the LoChro intervention, the authors also had the chance to watch two to three video documentaries on the LoChro interventions with the participant. During these videos, the participants prioritised and elaborated on their individual health problems.
Analysis of the healthcare situation of participants
The heterogeneity of clinical data, healthcare reports, video material and data from the questionnaires guided the choice of analytic method. Framework analysis was developed by Ritchie and Spencer in 1994 and has since been applied widely in health research.48 Framework analysis allows a systematic approach to be employed, being strongly based on study data, and is open to a greater variety of data types, in contrast to other approaches.48 49 Furthermore, the results of the framework analysis, from which the key themes are derived (see below), are transparent and can, as such, be further developed and discussed with patients, professionals, health policy makers and other stakeholders.
The research team consisted of three clinicians: a junior, intermediate and senior colleague. All analysts were familiar with public health research, one of them holding a Master’s Degree in Public Health. In addition, preresults were presented and discussed at the final LoChro advisory board meeting which was attended by different healthcare professionals, patient representatives and other stakeholders.
The framework analysis process
Framework analysis49 involved the following five steps:
(1) Familiarisation with the data. (2) Identifying recurring and important themes. (3) Indexing supporting examples from the data by matching themes that emerge from step 2. (4) Charting through the development of final key themes and subcategories. Subcategories are supported by data extraction using charts, one for each theme and a central chart, which includes all key themes and subcategories. (5) Analysis and Interpretation in which the key themes were brought into relation with the research question, reflecting on the results and embedding them into the existing knowledge base.
The following describes the process of framework analyses in this investigation in more detail:
For each case, data were sorted separately. All members of the research team independently worked through the data several times over, to familiarise themselves with the content and to get an overview of the whole process (step 1). Individual observations led to initial notes on recurring themes and the inter-relationships arising from patient data in the study group (step 2). To justify these recurring themes and their inter-relationships, the researchers selected specific data extractions (step 3). The researchers tried to avoid any a priori-labelling and to remain as unbiased as possible. In three workshops, their individual notes were then discussed. They aimed for greater validity, reliability and consistency by comparing their identified themes, their inter-relationships and their extracted data. Building key themes and subcategories involved debating the labelling, framing and reframing of themes and the rereading of data. Data extractions were also discussed, arranged and rearranged to affirm the emerging subcategories, key themes and their inter-relationships. Following these workshops, CS summarised the results obtained thus far through the use of charts for each key theme, with subcategories and data extractions combined into one central chart of all key themes and a figure to illustrate their inter-relationships. In a final workshop, the team discussed the charts and figure and, where necessary, reread the data. Finally, a consensus was reached and the final charts, as well as a final figure of their inter-relationships, were confirmed (steps 4 and 5).
Language
The language used for data collection and the framework analysis was German. Field notes were translated into English by a native speaking member of the study group (MS).
Ethical considerations
All methods were performed in accordance with relevant guidelines and regulations. Written informed consent was obtained from all participants or, if an individual had a legal representative, from the latter. Due to data protection concerns, the authors did not record any diagnoses or medication. Regarding descriptive results, if so, only broad outlines were presented.
Reporting this study followed the Standards for Reporting Qualitative Research published by O’Brien in 2014.50
Patient and public involvement
The LoChro trial design, materials and procedures including this qualitative investigation were discussed with patient representatives in a trial specific practice advisory board. After discussion they were adapted accordingly, and, moreover, after piloting the study process, all procedures were again adapted and, finally, approved by the LoChro practice and scientific advisory board.
Results
The healthcare situation of six older patients in southern Germany participating in the LoChro trial was evaluated over a period of 1 year. The six 1-year observation periods took place between 2018 and 2020.
The availability of the data differed between participants and different data sources. For all six participants, the data included discharge letters, medication plans, examination results and other reports from local hospital records. In all cases, the authors could evaluate the current outpatient medication regimes and the patient-reported answers to all the above-named questionnaires. In five cases, specialist reports from the outpatient sector were also present. Three of the cases also had comprehensive geriatric assessments. Unfortunately, none of the cases provided the authors with an insight into the GPs own notes.
The participants were aged between 70 and 85; the study included two female and four male participants. On average, the participants had 13 diagnoses each and took eight medications regularly per day. Each participant took at least one PIM and had at least one PPO. Table 1 lists further characteristics of the study population and the results of the PACIC.
Characteristics of the study population and results of the Patient Assessment of Chronic Illness Care (PACIC), (n=6)
Framework analysis
Five key themes were derived through analysis of the healthcare situations of the six multimorbid LoChro trial participants: Insufficient coordination of care, Overuse and Underuse of medical care, the Doctor’s role and the Patient’s role. Table 2 gives a summary of the key themes and their corresponding subcategories.
Key themes and corresponding subcategories of the healthcare situation of six multimorbid older persons in Germany
Insufficient coordination of care
In all six cases, the responsible professional for healthcare coordination was not properly stated. Responsibilities were also switched between healthcare providers without this being documented in the available data. The following examples illustrate the accountability breaks that the researchers found in the data. First, difficulties occurred in five of six cases when patients moved between the inpatient and the outpatient sectors (intersectoral responsibility): an outpatient specialist consultation was recommended several times by providers of the inpatient sector due to observed symptoms, without such a consultation taking place in the following 12 months. For a patient with a complex disease constellation, reviews were mainly organised by the hospital. However, treatments other than those for the main disease, that were still of relevance to the patient, were omitted. Second, responsibilities assigned to the outpatient sector, involving outpatient specialists and GPs, were also unclear (intrasectoral responsibility). One patient consulted several outpatient specialists as well as outpatient services of the local hospital, via the same specialty, leading to multiplication of expensive and redundant examinations. The coordination of the healthcare needs of another patient was mainly organised by the patient, which led to recommendations from differing healthcare providers. However, an overarching therapy plan was missing. In three of the six cases, a lack of communication of responsibilities led to delayed or missing drug prescriptions or other aspects of undersupply.
Overuse of medical services
Overuse of medical services occurred in redundant, partly unnecessary, healthcare contacts (high amount of doctor’s visits), PIM and redundant or overexamination. For example, one patient underwent one outpatient rehabilitation programme, as well as two inpatient stays, all referring to the same constellation of symptoms, without experiencing any improvement. All of the six participants took at least one PIM. However, in one case, specialists and the GP actively avoided overexamination, working actively together through regular communication and evaluating each other’s plans and examination results.
Underuse of medical services
Underuse was depicted through a lack of prevention/standard recommendations, PPOs and potentially missing assessments and/or examinations. Hence, five of six participants did not receive a vaccination against pneumococcus, although the indication according to the national vaccination committee51 was given. In all cases, PPOs were detected. Overall, assessment of fall risk, comorbidities including psychiatric and social needs were rarely documented. In one case, lifestyle advice as a measure of secondary prevention was lacking although the patient had previously demonstrated their ability for lifestyle change.
The doctor’s role
This was shaped by the subcategories explanation to the patient as one part of the shared decision-making process, the doctor’s anticipation of patient’s beliefs as well as limits such as time, financial or knowledge constraints. According to the participants (PACIC 1), therapy options were rarely elaborated on (mean (m) 20%; SD 19.0). For example, in the available care data, there was no evidence of a discussion of therapeutic options, and neither was there a discussion of therapeutic goals. An explanation of drug risk was documented at least once, with a focus on life-prolonging measures on the doctor’s part being seen in most cases. In one case, a neglect of secondary prevention related to the doctor’s belief that lifestyle modification was rejected by the patient. However, this assumption was neither confirmed nor discussed with the patient according to the information at hand. An effect of the healthcare situation due to time limits of the care providers was inferred in at least two cases. Further limits, such as financial or knowledge constraints, were not assessed directly. Yet, the lack of standard recommendations and the amount of PPOs indicated limits on the part of the care providers.
The patient’s role
Patient need, patient knowledge or other resources such as patient demand as well as patient satisfaction with healthcare formed the patient’s role. The care situation of one patient was shaped by their need for healthcare close to home. Another patient’s situation was affected by high symptom severity with frequent engagement of family members. In a third case, a care-intensive disease triggered a focus on the main disease. One patient who presented him/herself capable of introspection, reflection and self-management in the video material improved the care situation independently, but became overwhelmed with healthcare management in another situation. Overall, patient satisfaction with their healthcare was high, as patients stated 82% satisfaction with care on average on a 10-step Likert scale from 0% to 100% (PACIC 12: m 82%; SD 14.7).
Doctor–patient communication
The communication between doctor and patient refers to both key themes: the doctor’s role and the patient’s role. There were signs of shared decision-making, for example, one patient deciding to manage their diagnosis themselves. In another case, shared decision-making was well documented with regard to an invasive procedure. Participants reported that, in most cases, referrals to specialists were explained by the doctor (PACIC 11: m 33%; SD 34.4). However, most of the patients also stated that therapy options were rarely clarified (PACIC 1: m 20%; SD 19.0). Furthermore, apart from one case, documented shared decision-making could not be found. Out of the available data, it appeared that the patient focus was more on the ensuring of functional ability, while healthcare providers focused more on avoiding potential risks for medical events. Hence, a potential conflict in treatment goal was inferred, as several therapeutic choices were made without documented evidence of symptom improvement.
The inter-relationships between characteristics of the healthcare situations of the six study group patients
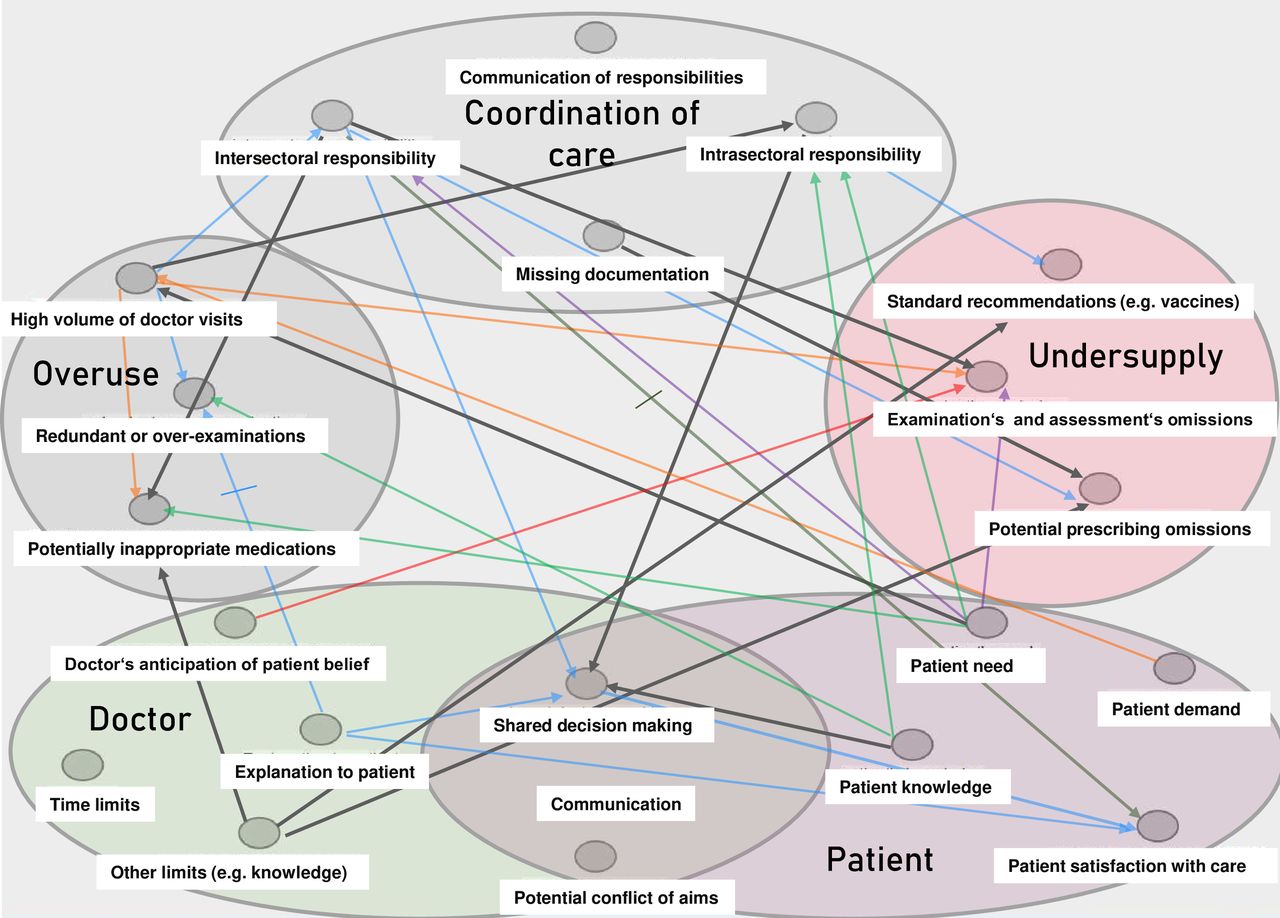
Figure 1 shows the inter-relationships between the key themes and corresponding subcategories that could be directly linked to the available data.

{kind=link}
Inter-relationships between key themes and subcategories of the healthcare situation of multimorbid older patients, seen in six underlying cases in Germany. Black arrows: repeatedly observed inter-relationships; coloured arrows: each colour stands for observations corresponding to one patient; crossed arrows: inhibiting relationship.
Ten chief inter-relationships can be inferred, as they occurred in more than one patient:
A high volume of doctor’s visits led to imprecise responsibilities within the outpatient sector: one patient consulted two colleagues of the same specialty regularly, which also led to redundant examinations. Another patient visited several doctors from different specialities, following different and sometimes contradictory treatment plans. Imprecise intersectoral responsibilities leading to an underuse of examination and assessment were, for example, reflected in a patient who had multiple inpatient visits to the same hospital for an oncological condition. In the video material, the patient pointed out that healthcare management shifted from the GP to the hospital. However, further patient statements, the hospital reports and data from outpatient carers highlighted that the treatment and secondary prevention of other life-threatening diseases had in the meantime been neglected. Another patient had experienced overtherapy, according to disease-specific guidelines for older patients in the inpatient setting. This in turn led to frequent changes in the treatment plan between the inpatient and outpatient sectors. Naturally, patient need, for example in terms of multiple continuing pathologies, led to a high volume of doctor visits. Two capable patients (patient knowledge) promoted shared decision-making, for instance by asking for the additional benefit of a computer tomography. Missing documentation of symptoms or diseases led to PPOs, and, assumed limits on the doctor’s part, as no other reasons were documented, leading to a lack of standard recommendations, such as vaccination against pneumococcus in almost all cases, PPOs and PIMs.
Discussion
This study describes the characteristics of the care situation of multimorbid older persons in southern Germany based on a 1-year analysis of six cases. Key themes that emerged from this analysis were insufficient coordination of care, overuse and underuse of care, and finally, the doctor’s role and the patient’s role. In addition, the study demonstrated inter-relationships between these key themes. Improved coordination of care with clarity of intersectoral and intrasectoral responsibilities arose as one of the main targets of future public health efforts, since overuse and underuse of healthcare as well as a lack of shared decision-making, were shown to be linked to insufficient coordination of care.
These findings are in accordance with other observations of the German healthcare system.26 The publication ‘Health system review: Germany’ (2020) describes ‘the strong separation of ambulatory and inpatient care in terms of organisation and payment, which can hinder the coordination and continuity of patient treatment’26 as being the primary challenge of the German health system. This study confirmed this remark by identifying insufficient coordination of care with the subcategories intersectoral and intrasectoral responsibility and communication as a key theme of the care situation of multimorbid older persons. In Germany, patients have a choice of GP, and can directly consult many ambulatory secondary care specialists without an official referral. In the absence of an officially regulated ‘gatekeeping’ system and with a traditionally strong separation of primary and secondary care, the ‘Health system review: Germany’ (2020) further emphasises that the lack in coordination of ambulatory care may be connected to a relatively high amount of available hospital admissions as demonstrated in the Organisation for Economic Co-operation and Development (OECD) Health at a Glance report 2021.26 52 Health policies established in Germany since the year 2000 targeted coordination of care within the ambulatory sector (subcategory intrasectoral care) and led to the establishment of diagnosis-specific Disease Management Programmes (DMP) in which documentation, patient information, referral indications and feedback reports were standardised. In 2021, the DMP was available for 10 diagnoses, however, multimorbidity was not included.53 Regionally regulated health conferences were implemented in which healthcare providers came together to discuss coordination challenges.54 However, on the patient level, only a few case conferences have taken place.26 A prospective matched cohort analysis of 208 patients could not demonstrate significant impacts of chronic care patient case conferences in primary care after 6 months.55 In addition, GPs reported the time to organise and coordinate these meetings as major barriers towards case conferences.56 Nonetheless, the present results strongly support efforts to strengthen coordination of care within the outpatient sector and across different sectors on the patient level, in addition to general management conferences and disease-specific programmes.
Overuse of medical services is often discussed in terms of medication oversupply57 (PIMs) or, otherwise, apparent oversupply which is concentrated on selected urban environments.58 However, Busse et al pointed out that the historic development of the German healthcare system starting with Bismarck’s reforms in 1883, had ‘led to an oversupply of pharmaceutical products, an excess in the number of inpatient cases and hospital stays, and problems with delivering continuity of care across sectoral boundaries’’.17 This study strengthens this notion as redundant inpatient stays as well as overuse of medical services in the ambulatory sector due to a lack of coordination could be demonstrated.
Underuse was also shown in this study. In addition, this was repeatedly associated with missing coordination of care. Not only were PPOs detected, but underuse occurred in the form of missing diagnostic information and delayed treatment. Strikingly, standard recommendations and prevention measures were severely neglected in the care of the participants of this survey. The latter may be in accordance with the German amount of preventable deaths being higher than many other European countries, for example Italy, Portugal and Greece.59
The doctor and patient roles, respectively, influenced the quality of care. The study sample provided signs of more reactive, less preventative medicine. This is in accordance with the most current healthcare trends, although a needs and research-driven shift towards more proactive medical management may be evolving.60 Qualitative and quantitative investigations into the doctor’s role caring for multimorbid patients28 61 are further indicators of the importance of these key themes. In Germany, however, there is little research on documentation within the GP setting. In contrast to other countries, patient information and documentation is not made available for evaluation from outside the practice. This is also reflected in the fact that GPs did not send their own notes for use in this study. Thus, only indirect inferences to limits of the doctor’s role could be made. Still, a lack of preventative measures, such as vaccination and secondary prevention, could be demonstrated via patient-reported data. This indicates that more research (a) on documentation in the GP practice and (b) on the reasons for potential insufficiencies in preventative care should be promoted to facilitate aids for improvement.
The analyses showed that older patients can and do act on behalf of their own healthcare providers. However, this needs guidance by a healthcare professional, capable of coordinating care. The promotion of health literacy,62 that was linked to shared decision-making in this study, is a further public health target.
Representativeness and limitations
The patients under investigation participated in the LoChro trial, thus belonging to a population with a high amount of multimorbidity. The average number of diagnoses (13; SD 3.8) and medications (8; SD 4.2) reflect this pattern. As shown in previous publications regarding the LoChro study group, participants had on average 13 diagnoses by inclusion, 10 of these documented in the hospital documentation system and three of these self-reported.63 Hence, the participants of this study were not representative of all elderly patients with multimorbidity in southern Germany, but might serve as examples for inferences of recurring healthcare themes.
This investigation has its limitations. First, data were not available in the requested amount, especially from GP practices where case notes were missing. This had implications for analysis as it remained partly unclear, whether, for example, an undersupply in the form of missed vaccinations was due to rejection by the patient or due to supply issues on the part of the doctor. However, the large amount of missed vaccinations reported in quantitative analyses of the LoChro study at baseline63 supported the notion that a lack of vaccination is associated with the doctor’s role. Also, communication with the patient who appeared to be omitted, might have been done verbally by the GP or another physician but not documented. Yet, the amount of available documentation, including correspondence between specialists and GPs over the course of a year, represents the part of healthcare documentation that is transparent, accessible and transferable between carers. This could help build the case for further care. Hence, documentation that was not available for this study may also be a hindrance to ease of access for healthcare workers. This lack of transparency represents a target for improvement. In addition, the patient perspective was provided mainly through answers to a questionnaire (PACIC) which, additionally, is prone to ground and ceiling effects.64 Only six cases were included in this in-depth investigation. However, the themes presented were reflected repeatedly in the six cases, so that saturation can be assumed for these themes. Furthermore, three of the six cases received the LoChro intervention, which may have had direct or indirect effects on the healthcare situation as the LoChro intervention aimed to strengthen patient self-management. However, no effect of the LoChro intervention on any of the primary or secondary outcomes, including a patient’s physical and mental well-being and patient satisfaction with their healthcare, could be demonstrated.40 Finally, all participants had been patients of the local university hospital, which implies good access to secondary and tertiary healthcare facilities, but lessens representativeness.
Conclusion
The investigation found insufficient coordination of care, overuse and underuse of medical services, as well as the doctor and patient role as recurring themes influencing the healthcare situation of multimorbid older patients. Regionally held case conferences under the eye of a single, clearly defined responsible party, should be evaluated further, as they could improve coordination of care. More specifically, advanced coordination of ambulatory care at the patient level should focus on avoiding1 redundant inpatient stays,2 overuse of outpatient services,3 the underuse of vaccinations and4 PPOs. The patient should be further supported through self-management strategies, however, with close guidance by their carers. To the best of author’s knowledge, this is the first investigation that directly links real-life cases to public health aspects of the care situation of multimorbid older patients in Germany. It may present us with opportunities to rethink and reorganise planning in healthcare, and could be of particular interest to research planners and decision-makers in the development of future healthcare-related policies.
Data availability statement
Data are available upon reasonable request. The data sets used and analysed during this study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethical committee of the University of Freiburg (ethical vote 495/17 on 28 November 2017). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors wish to thank all participants of the LoChro trial for their efforts spent in this research. We acknowledge support by the Open Access Publication Fund of the University of Freiburg.
References
Footnotes
Contributors CS, MS and AMa wrote the main manuscript text; CS, AMe and AMa performed the qualitative analysis; SV-R, as conceptual head of the LoChro trial, was responsible for the recruitment of participants and the whole study management, while GM and EF were responsible for data regarding patient satisfaction (PACIC) and patient’s health care use (FIMA). CS takes responsibility as guarantor and accepts full responsibility for the finished work and the conduct of the study, had access to the data, and controlled the decision to publish. All authors interpreted the data and read and approved the final manuscript.
Funding The LoChro-Trial was supported by the German Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung, BMBF). The grant number is: 01GL1703A.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.