Article Text

Abstract
Objectives To systematically assess the associations between various immune-mediated diseases (IMDs) and human papillomavirus (HPV)-associated diseases.
Design Retrospective cohort study.
Setting UK Biobank.
Participants A total of 500 371 subjects aged 40–69 years were eligible for the analysis, after excluding those with prevalent HPV-associated diseases at baseline and those who had withdrawn their informed consent or lacked information on sex.
Exposure Eighty IMDs (involving allergic/atopic diseases, autoimmune diseases, immunodeficiency diseases, etc) were identified in the UK Biobank.
Primary and secondary outcome measures The main outcome was the incidence of HPV-associated diseases (including warts and malignancies of the cervix, oropharynx, anus, penis, vulva and vagina). Cox proportional hazards model was used to estimate HRs and 95% CIs with particular adjustment for sexual behaviours. We also conducted subgroup analyses based on benign and malignant status, and anatomical sites of HPV-associated diseases, respectively.
Results During a median of 12.0 years of follow-up, 2244 cases out of 500 371 subjects developed HPV-associated diseases. Overall, participants with IMDs had a higher risk of HPV-associated diseases than their controls after adjustment for sexual behaviours and other potential confounders (female: HR=1.90, 95% CI=1.66 to 2.17, p<0.001; male: HR=1.66, 95% CI=1.41 to 1.97, p<0.001). Additionally, eight individual IMDs in women (eg, asthma: HR=1.76, 95% CI=1.47 to 2.11, p<0.001) and three in men (eg, chronic nephritic syndrome: HR=6.05, 95% CI=3.32 to 11.04, p<0.001) were associated with increased risk of HPV-associated diseases. Subgroup analyses revealed significant IMD differences between benign and malignant subgroups as well as between oropharyngeal and anogenital subgroups.
Conclusion In this large retrospective cohort study, IMDs were significantly associated with an elevated risk of HPV-associated diseases. Besides, gender-specific and region-specific associations were also observed between individual IMDs and HPV-associated diseases.
- EPIDEMIOLOGY
- IMMUNOLOGY
- VIROLOGY
- DERMATOLOGY
- ONCOLOGY
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
To the best of our knowledge, this is the largest retrospective cohort to date exploring the association of immune-mediated diseases (IMDs) with human papillomavirus (HPV)-associated diseases.
Comprehensive subgroup analyses based on anatomical sites and benign and malignant nature of HPV-associated diseases were conducted and a wide range of important confounders were considered.
As IMDs were ascertained through hospital records, people with undiagnosed IMDs may have been missed.
The medications for IMD treatment were not adjusted for the observed associations due to the limited sample sizes of certain individual IMDs.
HPV-associated diseases were identified based on their acknowledged relationships with HPV infection, not a positive HPV test result, which might cause a confounding effect on our findings.
Introduction
Immune-mediated diseases (IMDs) represent a highly heterogeneous group of pathologies, posing heavy burden on medical insurance worldwide.1 The development of IMDs is considered as the consequence of multiplex interaction between environmental and genetic factors, which trigger the immune dysregulation and result in subsequent systemic or organ-specific injuries.2 Previous studies have revealed common susceptibility loci and pathways behind the co-occurrence of certain IMDs, indicating similar patterns of comorbidity and clinical outcomes might also be shared between them.2 3
Human papillomavirus (HPV), one of the most common sexually transmitted infections, is estimated to infect nearly all sexually active women at least once in their lifetime.4 HPV initially invades the skin and mucosa, of which the persistent infection has been confirmed to be a major causative factor of a series of HPV-associated diseases, including benign skin warts and malignancies originating from the head and neck region as well as anogenital organs.5 Various immune cells in both the circulation and local tissues, especially regulatory T cells, are involved in the host response to HPV infection, which play pivotal roles in shaping immunosuppressive microenvironment and promoting the gradual formation of neoplasm.6 7 These findings suggest a sophisticated immune-mediated pathogenic network of HPV-associated diseases.
Previous studies had demonstrated higher rates of HPV infection among patients with certain IMDs, including psoriasis and multiple rheumatic diseases.8 9 Meanwhile, reduced immune-mediated eradication and abnormal inflammatory microenvironment have been shown to promote HPV-induced carcinogenesis, indicating the importance of immune dysregulation in developing HPV-associated diseases.6 10 However, few studies have investigated the associations between IMDs and HPV-associated diseases. Therefore, in this study, we aimed to systematically explore the association of various IMDs with the risk of HPV-associated diseases based on UK Biobank (UKB) cohort data. We also conducted subgroup analyses by anatomical sites and differences between benign and malignant diseases, respectively.
Methods
Study design and participants
This retrospective cohort study leveraged data from the UKB, a national database that recruited over 500 000 adults in the UK during 2006–2010, which aimed to explore the genetic, lifestyle and environmental determinants of a wide range of diseases.11 12
For this study, participants with prevalent HPV-associated diseases at baseline (n=1960) and those who had withdrawn their informed consent (n=158) and lacked information on sex (n=1) were excluded from the study (figure 1).

Study flow chart. HPV, human papillomavirus; IMDs, immune-mediated diseases.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Ascertainment of IMDs
A total of 80 IMDs (involving various allergic/atopic diseases, autoimmune diseases, immunodeficiency diseases, organ transplantation, etc) were identified using the International Statistical Classification of Diseases and Related Health Problems 10th version (ICD-10) codes (online supplemental table 1). We initially examined whether the risk of HPV-associated diseases differs between participants with and without any IMDs on the holistic level. In terms of the subsequent analysis of individual IMD, only those with more than 100 affected individuals and at least 10 corresponding incident cases (ie, total, benign, malignant, oropharyngeal, anogenital, cervical HPV-associated diseases, respectively, as described below) were taken into account to improve the reliability of results.
Supplemental material
Outcome ascertainment
The primary outcome was the diagnosis of HPV-associated diseases (including benign warts and malignancies of the cervix, oropharynx, anus, penis, vulva and vagina), which was ascertained through data linkage with national electronic administrative health records, with corresponding ICD-10 codes presented in online supplemental table 2. All analyses were performed separately for men and women since specific HPV-associated diseases differed in men (including penile, anal and oropharyngeal cancers, and warts) and women (including cervical, vaginal, vulvar, anal and oropharyngeal cancers, and warts).
We also conducted subgroup analyses based on differences between benign and malignant diseases, and anatomical sites, respectively. Briefly, the total HPV-associated diseases were divided into benign and malignant categories, the former including warts and the latter including all related malignancies which could be further categorised by anatomical sites as oropharyngeal cancer and anogenital cancer (penile and anal cancers in men, and vaginal, vulvar, cervical and anal cancers in women). Besides, cervical cancer was specifically analysed due to its clinical importance and large sample size, while other individual tumours were not analysed separately due to the limited sample sizes. All diagnoses were identified at the date when their ICD-10 codes were first recorded. We defined incident cases of HPV-associated diseases as individuals with a diagnosis present at least 12 months after the diagnosis of IMDs.
Statistical analysis
All study participants were followed up from the date of baseline assessment to either the date of HPV-associated diseases diagnosis, death, loss to follow-up or the end of the data linkage (16 March 2021), whichever came first. The exposure group was composed of subjects with prevalent IMDs at recruitment and those who reported incident disease diagnosis during the follow-up period.
Normality was assessed by Cramer-von Mises test. The baseline characteristics of participants with and without incident HPV-associated diseases were summarised using the means with SDs and median (IQR) for quantitative variables, and percentages for categorical variables. Χ2 test or Fisher’s exact test was used to compare the difference between categorical variables, while the Student’s t-test or the Wilcoxon rank-sum test was applied to evaluate the continuous variables, as appropriate.
Univariate and multivariable Cox proportional hazards models were used to estimate HRs and 95% CIs for the relationships between total/individual IMDs and the risk of total/benign/malignant/oropharyngeal/anogenital/cervical HPV-associated diseases. In multivariable analysis, we constructed four incremental models for each outcome: model 1 (minimally adjusted) was adjusted for age and ethnicity; model 2 was additionally adjusted for socioeconomic status (Townsend deprivation score); model 3 was further adjusted for smoking status and alcohol drinker status; model 4 (maximally adjusted) was adjusted for all covariates in model 3 as well as lifetime number of sexual partners and same-sex behaviour. Participants with any missing data are excluded from further analysis.
All statistical analyses were conducted using R software (V.3.6.3) together with add-on packages. Statistical tests were two sided with a p value of <0.05 considered as statistically significant, but when further comparing the risk of developing HPV-associated diseases between individuals with and without IMDs, we deemed the p value of <0.001 as statistically significant to reduce the likelihood that the resulting test statistic was obtained by chance and make the observed associations more reliable.
Results
Baseline characteristics
A total of 500 371 subjects (mean (SD) age, 56.5 (8.1) years/median (IQR) age, 58.0 (50.0–63.0) years) were included in this study, of which 271 817 (54%) were female and the vast majority (95%) were white. As shown in table 1, compared with those without incident HPV-associated diseases, participants with incident HPV-associated diseases were more likely to be older, white, socioeconomically deprived and less educated. Besides, participants with incident HPV-associated diseases were more likely to have an unhealthy lifestyle, represented by current smoking and alcohol consumption (women), and were more sexually active, for example, having ≥6 lifetime sexual partners and an earlier age at first intercourse. Specifically, male participants with incident HPV-associated diseases tended to have same-sex behaviour, ≥6 lifetime same-sexual partners and a history of aspirin use, compared with their counterparts. More detailed comparison of baseline characteristics between individuals with and without benign/malignant/oropharyngeal/anogenital/cervical HPV-associated diseases was presented inonline supplemental tables 3–6.
Clinical and demographic characteristics of all study subjects by sex (n=500 371)
IMDs and risk of total HPV-associated diseases
During a median follow-up of 12.0 years, a total of 2244 incident cases (1302 women; 942 men; incidence rate: 0.40 per 1000 person-years) with HPV-associated diseases were identified. Overall, IMDs were significantly associated with an increased risk of HPV-associated diseases, with a multivariable-adjusted HR of 1.90 (95% CI: 1.66 to 2.17, p<0.001) in female participants and 1.66 (95% CI: 1.41 to 1.97, p<0.001) in male participants for total HPV-associated diseases (table 2 and figure 2).
Associations between IMDs and the risk of HPV-associated diseases by sex

{kind=link}
{kind=link}
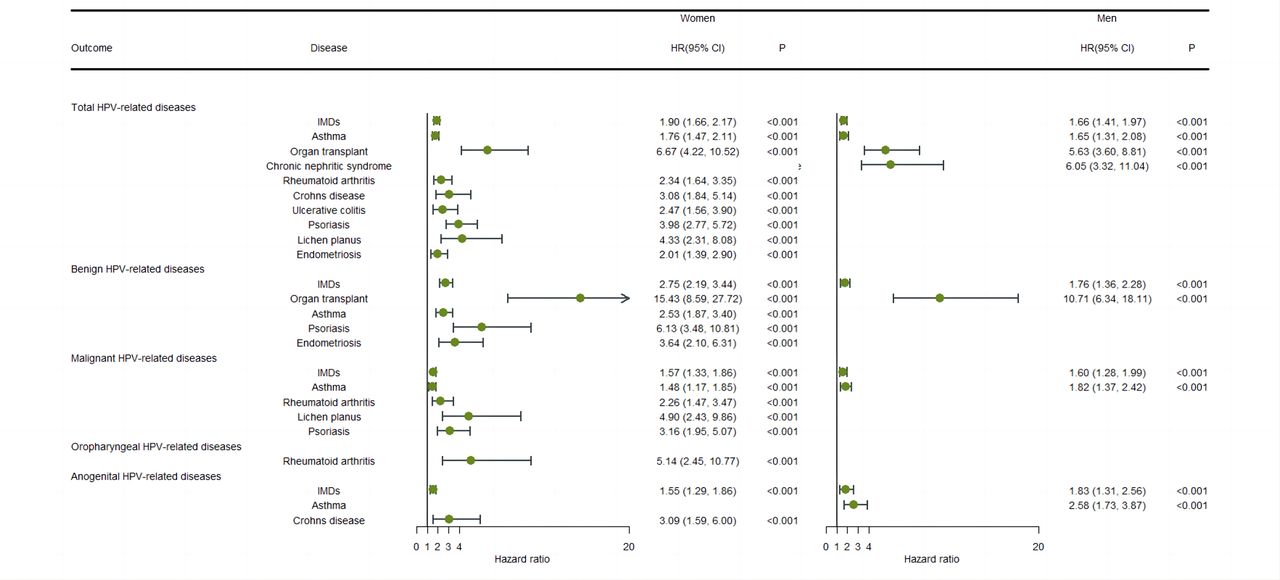
Forest plot summarising the associations of IMDs with risk of HPV-associated diseases by sex. Data are presented as HR and 95% CI. The analyses were adjusted for age, ethnicity, socioeconomic status (Townsend deprivation score), smoking status, alcohol drinker status, lifetime number of sexual partners and same-sex behaviour (model 4). ‘IMDs’ refers to compare the outcome risk between participants with at least 1 of 80 IMDs and those without any IMDs. HPV, human papillomavirus; IMDs, immune-mediated diseases.
Among female participants, a total of nine individual IMDs were positively associated with the risk of overall HPV-associated diseases in the univariate model (online supplemental table 7), of which eight individual IMDs still remained significant after adjustment for age, ethnicity, socioeconomic status, smoking status, alcohol drinker status, lifetime number of sexual partners and same-sex behaviour (model 4). More specifically, female participants with asthma (HR=1.76; 95% CI: 1.47 to 2.11, p<0.001), organ transplant (HR=6.67; 95% CI: 4.22 to 10.52, p<0.001), rheumatoid arthritis (HR=2.34; 95% CI: 1.64 to 3.35, p<0.001), Crohn’s disease (HR=3.08; 95% CI: 1.84 to 5.14, p<0.001), ulcerative colitis (HR=2.47; 95% CI: 1.56 to 3.90, p<0.001), psoriasis (HR=3.98; 95% CI: 2.77 to 5.72, p<0.001), lichen planus (HR=4.33; 95% CI: 2.31 to 8.08, p<0.001) and endometriosis (HR=2.01; 95% CI: 1.39 to 2.90, p<0.001) were at increased risk of developing HPV-associated diseases (table 2 and figure 2).
On the other hand, among male participants, those diagnosed with asthma (HR=1.65; 95% CI: 1.31 to 2.08, p<0.001), organ transplant (HR=5.63; 95% CI: 3.60 to 8.81, p<0.001) or chronic nephritic syndrome (HR=6.05; 95% CI: 3.32 to 11.04, p<0.001) had a higher risk of total HPV-associated diseases compared with their counterparts (table 2 and figure 2).
Subgroup analyses based on the differences between benign and malignant HPV-associated diseases
Subgroup analyses by sex for benign and malignant HPV-associated diseases remained statistically significant, in which female participants with IMDs were under a higher risk of developing both benign (HR=2.75, 95% CI: 2.19 to 3.44, p<0.001) and malignant (HR=1.57, 95% CI: 1.33 to 1.86, p<0.001) HPV-associated diseases. Similar associations were also observed in male participants (HR=1.76, 95% CI: 1.36 to 2.28, p<0.001 for benign HPV-associated diseases and HR=1.60, 95% CI: 1.28 to 1.99, p<0.001 for malignant HPV-associated diseases) (table 2 and figure 2).
Furthermore, we observed that organ transplant (HR=15.43; 95% CI: 8.59 to 27.72, p<0.001), asthma (HR=2.53; 95% CI: 1.87 to 3.40, p<0.001), psoriasis (HR=6.13; 95% CI: 3.48 to 10.81, p<0.001) and endometriosis (HR=3.64; 95% CI: 2.10 to 6.31, p<0.001) were significantly associated with an increased risk of developing warts across all unadjusted and multivariable-adjusted models (models 1–4) in female participants, whereas only organ transplant (HR=10.71; 95% CI: 6.34 to 18.11, p<0.001) seemed to be associated with an increased risk of developing warts in male participants (online supplemental tables 7–9; table 2 and figure 2).
Meanwhile, results derived from the maximally adjusted model (model 4) performed in female participants indicated that asthma (HR=1.48; 95% CI: 1.17 to 1.85, p<0.001), rheumatoid arthritis (HR=2.26; 95% CI: 1.47 to 3.47, p<0.001), lichen planus (HR=4.90; 95% CI: 2.43 to 9.86, p<0.001) and psoriasis (HR=3.16; 95% CI: 1.97 to 5.07, p<0.001) were all risk factors for HPV-associated malignancies, with asthma (HR=1.82; 95% CI: 1.37 to 2.42, p<0.001) being a risk factor in men as well.
Subgroup analyses based on anatomical sites of HPV-associated diseases
Subgroup analyses by sex for anatomical sites of HPV-associated diseases showed that female participants with IMDs were under a higher risk of developing anogenital HPV-associated diseases (HR=1.55, 95% CI: 1.29 to 1.86, p<0.001). Similar associations were also observed in male participants (HR=1.83, 95% CI: 1.31 to 2.56, p<0.001 for anogenital HPV-associated diseases). Additionally, we have not observed any significant association between IMDs and cervical HPV-associated diseases in female participants (table 2 and figure 2).
Furthermore, we observed that rheumatoid arthritis (HR=5.14; 95% CI: 2.45 to 10.77, p<0.001) was strongly linked with an increased risk of developing oropharyngeal cancer in female participants. Besides, Crohn’s disease (HR=3.09; 95% CI: 1.59 to 6.00, p<0.001) conferred an increased risk of anogenital HPV-associated malignancies in women, whereas among male participants, only asthma (HR=2.58; 95% CI: 1.73 to 3.87, p<0.001) showed a statistically significant association with anogenital HPV-associated malignancies after adjusting for potential confounding factors in model 4 (table 2 and figure 2).
Discussion
In the present study, we observed significant associations of IMDs with increased risk of total HPV-associated diseases in both female and male participants after adjusting for demographic characteristics, common cancer risk factors and history of sexual behaviours. Gender-specific associations were observed between individual IMDs and total HPV-associated diseases, in which more types of IMDs were found to be significantly associated with increased risk of HPV-associated diseases in female participants (asthma, organ transplant, rheumatoid arthritis, Crohn’s disease, ulcerative colitis, psoriasis, lichen planus and endometriosis) compared with male participants (asthma, organ transplant and chronic nephritic syndrome).
Besides, subgroup analyses revealed significant differences between IMD panels associated with the risk of HPV-associated diseases. Specifically, among female participants, asthma and psoriasis were significantly associated with increased risk of both benign and malignant HPV-associated diseases; organ transplant and endometriosis were only associated with increased risk of benign HPV-associated diseases, while rheumatoid arthritis and lichen planus were only associated with increased risk of malignant HPV-associated diseases. On the other hand, rheumatoid arthritis was significantly associated with increased risk of oropharyngeal HPV-associated diseases, whereas Crohn’s disease was associated with increased risk of anogenital HPV-associated diseases. Nevertheless, among male participants, only organ transplant was found to be associated with increased risk of benign HPV-associated diseases, while only asthma was associated with increased risk of malignant HPV-associated diseases. Meanwhile, only asthma was associated with increased risk of anogenital HPV-associated diseases, whereas no individual IMD was identified to be associated with oropharyngeal HPV-associated diseases. Our findings might provide insight into the local and systemic effects of IMDs in the development of HPV-associated diseases.
Specifically, asthma was found to be associated with increased risk of both benign and malignant HPV-associated diseases in female participants. Previous studies have shown that the dysregulation of innate immune system in patients with asthma could contribute to the alternated incidence of various types of cancer,13 14 which is partially consistent with our results. Asthma is characterised by the upregulation of T helper cells (Th)2 immune response and the downregulation of Th1 response, which might contribute to the formation of HPV-induced immunosuppressive microenvironment and thus promoting the gradual formation of neoplasm.15
Nevertheless, only female participants with psoriasis were more likely to develop both benign and malignant HPV-associated diseases, highlighting the gender influence on the immune regulation of systemic IMDs. Previous studies have shown that the prevalence of HPV infection was higher in patients with psoriasis under immunosuppressive treatment or biotherapy, and the incidence of HPV-associated diseases might therefore increase.9 16 17 These findings suggest that special attention should be paid to prevent patients with IMD from receiving systemic therapy from HPV infection.
Notably, inflammatory bowel diseases (IBDs) showed strong association with the increased risk of anogenital HPV-associated diseases, suggesting a pivotal role of extended carcinogenic effect for nearby structures. Numerous studies have demonstrated the association of IBDs with both local and extralocal neoplasms, which could be explained by the combination of both chronic inflammatory microenvironment and systemic immune suppression resulting from systemic therapy.18–21
To the best of our knowledge, this is the largest retrospective cohort assessing the association between IMDs and HPV-associated diseases. Besides, we have also conducted comprehensive subgroup analyses based on anatomical sites and benign and malignant nature of HPV-associated diseases. In addition, we further adjusted for history of sexual behaviours, which were potential confounding factors. However, there are also some limitations in this study. First, limited by the sample sizes of certain individual IMDs, the medications for IMD treatment were not adjusted for the observed associations. However, a recent prospective study of a large sample size has shown that the medications for IMD treatment were not associated with cancer risk.14 Second, the diagnoses of IMDs in this study were retrieved through hospital-diagnosed ICD-10 codes, which might result in the ignorance of some undiagnosed patients with IMDs who have not received formal medical service. Nevertheless, the prevalence of IMDs in our study seemed to be consistent with previous studies.1 14 22 Third, due to the limited information, HPV-associated diseases in this study were identified on the basis of their acknowledged relationships with HPV infection, not a positive HPV test result, which might cause a confounding effect on our findings. However, the confirmed high prevalence of HPV infection in these diseases could assure that the trends observed in this study are relatively reliable.
Conclusion
In this long-term retrospective cohort study, we observed that overall and certain individual IMDs were significantly associated with increased risk of HPV-associated diseases. Besides, gender-specific and region-specific associations were observed between individual IMDs and HPV-associated diseases. Our findings might provide insight into the local and systemic immunoregulation in the development of HPV-associated diseases, indicating that special attention should be paid to prevent certain patients with IMDs from having HPV infection.
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
The generic ethical approval of the UK Biobank Study was granted by the NHS North West Multicentre Research Ethics Committee and the National Information Governance Board for Health and Social Care (ref: 11/NW/0382). All participants provided written informed consent for data collection, analysis and linkage, which could be withdrawn at any time. Further details of data collection procedures are publicly available in the UK Biobank (http://www.ukbiobank.ac.uk/wp-content/uploads/2011/11/UK-Biobank-Protocol.pdf.). Our current study was approved by the UK Biobank research committee (approval ID: 69718).
Acknowledgments
This research has been conducted using the UK Biobank resource under application number 69718. We would like to thank all participants for their contribution to this research.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
LF, KQ and YR contributed equally.
Contributors This work was completed collaboratively by a team of researchers with diverse backgrounds and areas of expertise. Each author has made significant contributions to the research project and the writing of the manuscript. Following are the specific roles for each author: LF—study planning, design, data collection and analysis, results interpretation and manuscript write-up. KQ—study planning, design, results interpretation and manuscript write-up. YR—study planning, design, data collection and analysis, and manuscript write-up. TS—study planning, design, data extraction and statistical analyses. YS—literature search and manuscript write-up. DC—study planning, design, literature search and screening. MM—data collection and results interpretation. JL—data analysis and results interpretation. ZZ—data extraction and analysis. XW—data extraction and analysis. XZ—data extraction and analysis. YZ—study planning, design, supervision and reviewing the final report. JR—the guarantor, study planning, design, supervision and making critical revision of the manuscript.
Funding This work was supported by the National Natural Youth Science Foundation of China (grant numbers 82002868 and 82272777); West China Hospital, Sichuan University (grant number ZYJC21027); the Science and Technology Department of Sichuan Province (grant numbers 2022YFS0066 and 2021YFS0156); and Sichuan Medical and Health Care Promotion Institute (grant number KY2022QN0270).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.