Article Text

Abstract
Objectives Human papillomavirus (HPV) infection is closely associated with cervical cancer, especially the persistent infection of high-risk HPV (HR-HPV) genotypes. Therefore, investigating the HPV prevalence, age-specific, genotype distribution and the impact of the COVID-19 pandemic among large populations was essential for HPV screening and optimising vaccination.
Design This was a cross-sectional study.
Methods A total of 38 056 cervical epithelial cell specimens were collected in Weifang city from January 2018 to December 2022. The study was divided into seven age groups based on the age of the participants. HPV genotype testing was performed by using a commercial kit which is designed for the detection of 23 HPV genotypes.
Result A total of 8998 women were infected with HPV, with an overall positive rate of 23.64% (8998/38 056). Single infection of HPV was dominant among different age groups, which accounted for 71.33% of total infections. The most prevalent genotype was HR-HPV 16 (4.33%), followed by 52, 58, 53 and 68. Low-risk HPV (LR-HPV) 42 exhibited the highest prevalence (2.19%) among six LR-HPV genotypes, representing a novel finding. There was a significant difference in the prevalence across different age groups (p<0.01), with the highest prevalence in the group under 25 years old. During the 3 year COVID-19 breakout period, the number of HPV samples received in 2020, 2021 and 2022 was reduced by 24.03%, 14.79% and 24.76%, respectively. In 2018–2022, the annual prevalence varied between 21.09% and 25.30%, with a decreasing trend, while the prevalence of HR-HPV 39, 56, 31 and LR-HPV 42 increased.
Conclusion This study indicates a high-HPV infection rate and age-specific distribution characteristics of HPV genotype infections, as well as analyses of the impact of the COVID-19 outbreak on the HPV prevalence, which provides an epidemiological basis for the control and prevention of HPV infection in this region.
- VIROLOGY
- Molecular biology
- COVID-19
- Infectious diseases & infestations
Data availability statement
Data are available on reasonable request. The data sets used and/or analysed during this study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This is the first study on the prevalence and distribution of human papillomavirus (HPV) genotypes in women in Weifang, China.
This study analysed the impact of the COVID-19 pandemic on HPV prevalence among women.
Data for genotypes 81 and 82 were not obtained in 2018 because these two genotypes were not included in the testing kit for this year.
Introduction
Human papillomavirus (HPV) is a small double-stranded circular DNA virus with multiple genotypes.1 More than 200 HPV genotypes have been identified by DNA data analysis, among which about 40 HPV genotypes are involved in reproductive tract infection,2 and the infection is widespread in the crowd.3 According to the carcinogenic potential, these HPV genotypes were divided into HR-HPV genotypes and LR-HPV genotypes.4 The International Agency for Research on Cancer (IARC) classified 12 HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58 and 59) in group 1 and 1 HPV type (68) in group 2A as HR-HPV types. In addition, group 2B also includes HPV types 26, 53, 66, 67, 70, 73 and 82, with limited evidence in humans for cervical cancer.5 Up to 70% of cervical cancer are caused by HPV 16 and HPV 18, with HPV 16 being the most prevalent;6 additionally, genital skin and mucous membrane are frequently affected by LR-HPV genotypes such as HPV 6, 11, 40, 42, 43, 44, 54, 55 and so on.7 HR-HPV genotypes persistent infection is the main cause of cervical cancer,8 which is the fourth most common cancer among women worldwide,9 and a study reported that the rate of HPV infection in cervical cancer patients could be as high as 99.7%.10
At present, the HPV vaccine plays a key role in reducing the mortality of cervical cancer and releasing the burden of HPV infection, making a significant contribution to the prevention of cervical cancer in some developing countries.11 There are three types of HPV vaccines available in Shandong province: the bivalent HPV vaccine contains virus-like particles (VLPs) against HR-HPV types 16 and 18; the quadrivalent vaccine contains VLPs HPV types 6, 11, 16 and 18 and the nonavalent HPV vaccine contains VLPs against HPV types 6, 11, 16, 18, 31, 33, 45, 52 and 58. Currently, only the domestic bivalent HPV vaccine is approved by National Medical Products Administration (https://www.nmpa.gov.cn/datasearch/search-result.html) in China. Therefore, the quadrivalent and nonavalent HPV vaccines need to be imported completely, which is not only expensive but also the genotypes that can be prevented may not be wholly consistent with the genotypes that Chinese people are susceptible to. Meanwhile, due to the differences in climate, age, living habits and population distribution, there are regional variations in cervical HPV infection rate and genotype distribution among women in different regions.12 Therefore, prevention and control measures for HPV infection should be implemented according to their local situation. So, a full investigation of the local HPV prevalence and genotype distribution is important for developing strategies to prevent and control HPV.
From the beginning of 2020 to the end of 2022, China has implemented strict lockdown measures and limited physical contact to prevent the spread of COVID-19. Although the fact that these measures have proved to be efficient for the control of respiratory virus infections, the incidence of several sexually transmitted infections, such as syphilis, chlamydia and gonorrhoea, has also decreased.13 14 Did these measures taken during the COVID-19 pandemic have an impact on the prevalence of HPV infection? This study statistically analysed HPV testing data before and after the COVID-19 epidemic, aiming to investigate the 5 years HPV infection characteristics, including HPV infection rate, infection genotypes, age distribution and annual infection, also investigated the impact of COVID-19 on the prevalence of HPV during the pandemic. Therefore, the results of the analysis of HPV 23 genotypes in cervical epithelial cell specimens of 38 056 women from 2018 to 2022 are as follows.
Materials and methods
Study design
This study was a cross-sectional study. We collected large-scale cervical epithelial cell specimens from female patients who attended the health examination centre and gynaecological outpatient clinics in our hospital from January 2018 to December 2022. All samples were stored at 4°C and then transported to the molecular biology laboratory; subsequent HPV genotype testing was performed within 24 hours. The number of specimens in the area during the study period determined the sample size.
Patient and public involvement
The inclusion criteria for the study were as follows: outpatient and inpatient women who were attending first-time HPV types testing and were living in the selected Weifang area. A total of 38 056 eligible women were included. Patients and the public were not further involved in the implementation of this study.
HPV genotype testing
Anadas 9850 was used to extract and amplify HPV DNA, which was a fully automatic nucleic acid extraction and real-time PCR analysis system (Amplly Biotechnology Co., Xiamen, China). HPV DNA was extracted by a Magnetic-based Nucleic Acid Extraction Kit (APL-HSTQ1701) (Amplly Biotechnology Co., Xiamen, China). HPV genotypes were tested by Genotyping Nucleic Acid Detection Kit (A215420200811) (Amplly Biotechnology Co., Xiamen, China). This multiple real-time PCR amplification kit could detect 13 HR-HPV genotypes, four possibly carcinogenic types and six LR-HPV genotypes via gene amplification technology and diversion hybridisation. The amplification was performed under the following conditions: 38°C predenaturation for 5 min, then 95°C denaturation for 2 min, followed by 40 cycles at 95°C for 10 s, 58°C for 50 s (fluorescence signal collection was set at 58°C for 30 s). The lowest limit of detection was 500 copies/mL, if HPV DNA load is greater than or equal to 500 copies/mL, then defined as positive. HPV viral DNA extraction, real-time PCR amplification and result interpretation were performed according to the manufacturer’s instructions. Quality controls of HPV genotype testing including external quality assessment (negative control and positive control) and internal quality control were implemented throughout the study. Internal quality control was used to ensure that the cervical epithelial cells had been collected.
Statistical analysis
All statistical analyses were performed using Excel 2019 and SPSS V.25.0 software (IBM Corp., Armonk, NY, USA). The distribution of HPV genotype was expressed using indicators such as infection rate and prevalence (%). The 95% CI was estimated for each calculation to get the prevalence of HPV. The difference between prevalence, genotype and number of coinfections of HPV in different age groups and time groups was evaluated by Pearson’s χ2 test. For all statistical analyses, p values were two-sided and p<0.05 was considered statistically significant.
Time trend analysis was performed using Joinpoint Regression Programme V.5.0.2. The data that were not obtained in 2018 were not analysed.
The age of screened participants ranged from 14 to 84 years old, and the mean age was 40.38±11.67 years. They were divided into seven groups, each covering a 10 year range: T1 group indicates age <25; T2 group indicates 25≤age<35; T3 group indicates 35≤age<45; T4 group indicates 45≤age<55; T5 group indicates 55≤age<66; T6 group indicates 65≤age<75 and T7 group indicates age≥75.
Results
Overall HPV prevalence and genotype distribution
In this study, a total of 38 056 samples from female participants were collected between 2018 and 2022, among which 8998 women were screened positive for HPV, with an overall HPV infection rate of 23.64% (95% CI, 23.22 to 24.07, as shown in table 1). Furthermore, among these positive infections, 2580 women were positive for multiple infections, including 1758 patients with double infections, 538 patients with triple infections, 178 patients with quadruple infections and 106 patients with more than quintuple or sextuple infections. The constituent ratio of overall infection, single infection, and multiple infections of HPV-positive are shown in figure 1A.

Overall HPV prevalence and genotype distribution. (A) Constituent ratio of HPV infection. (B) The prevalence of both 23 HPV types infection rate in 38 056 women. HPV, human papillomavirus.
Comparison of annual total, single and multiple prevalence of HPV from 2018 to 2022
As shown in figure 1B, the most prevalent genotype was HPV 16 with the highest infection rate of 4.3% (95% CI, 4.12 to 4.53) (1646/38 056). The remaining types of high-risk or possibly carcinogenic were listed in descending order: HPV 52 (3.93%), 58 (3.02%), 53 (2.14%), 68 (1.42%), 56 (1.41%), 31 (1.31%), 66 (1.26%), 51 (1.22%), 39 (1.20%), 33 (1.19%), 18 (1.17%), 59 (1.16%), 35 (0.52%), 45 (0.40%), 82 (0.37%) and 73 (0.27%). Furthermore, positive women for HPV 16 occupied 18.29% of 8998 HPV-positive participants, that is, the ratio-in-positive for HPV 16 was 18.29% (1646/8998). However, among the multiple infection genotypes, HPV 52 was detected most frequently with infection rate of 2.47% (939/38 056). In addition, the infection rates of common LR-HPV genotypes were in decreasing order: HPV 42 (2.19%, 835/38 056), HPV 43 (1.45%, 551/38 056), HPV 81 (1.17%, 444/38 056), HPV 44 (1.06%, 405/38 056), HPV 6 (1.01%, 384/38 056) and HPV 11 (0.67%, 257/38 056).
Distribution characteristics of different age groups
A total of 38 056 female participants of HPV were divided into seven age groups according to their ages at the time of genotype testing. Both single and multiple infection rates of HPV with different age groups are shown in figure 2. According to the total infection as displayed, there was a significant difference in the prevalence across the different age groups (p<0.01). The women who were younger than 25 years had the highest HPV prevalence 36.74% (697/1897, 95% CI: 34.57 to 38.91), after then there was a declining trend in the middle age groups, but the prevalence of HPV in 35≤age<45 and 55≤age<65 age groups was a slight increase, respectively (figure 2, line a). Single infection was the most common infection pattern in all age groups (figure 2, line b). The prevalence of multiple infections and HR-HPV 16 are shown in line c and line d, respectively. As shown in online supplemental table S1, the proportion of positives was 53.08% in the group under 25 years old, and grew steadily to reach its highest in the 35–44 year group (76.06%), and then gradually decreased as age increased (except for age group above 75 years). In terms of multiple infections, double infections accounted for the largest proportion and peaked in two age groups (under 25 years and 55–64 years), with 23.38% and 23.23%, respectively. It is noteworthy that the proportion gradually declines in groups T1, T2 and T3 (age<44 years) and starts to increase in groups T4 and T5 (age from 45 to 64 years) both in double, triple and quadruple HPV genotype infections.
Supplemental material

Prevalence of HPV infection in different age groups with 95% CI bars. HPV, human papillomavirus.
The proportion of HPV genotype in different age groups among 8998 women
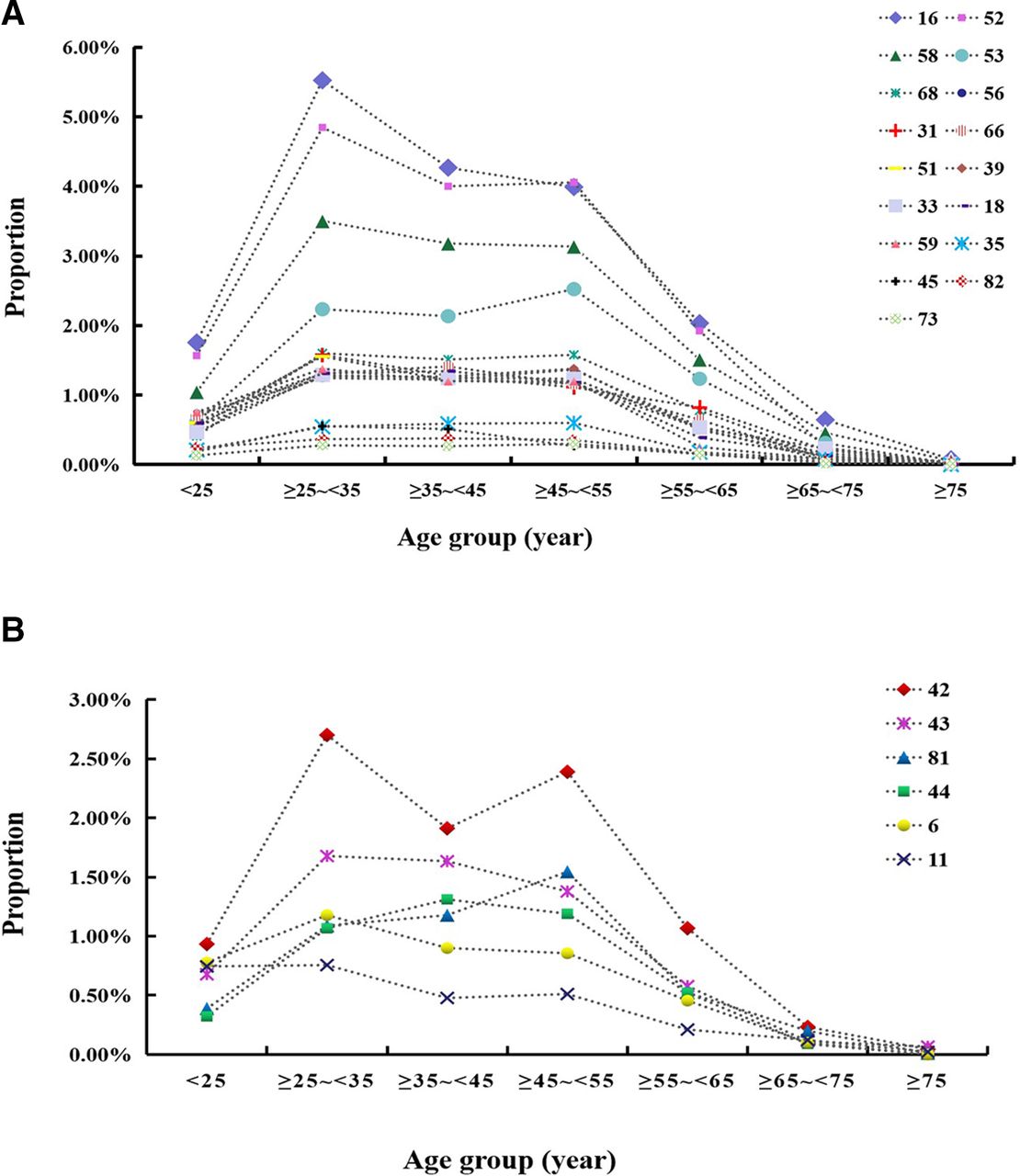
Figure 3A,B reveals the proportion of positives for HPV genotypes in different age groups among HPV-positive females. In this study, the positives for all HPV genotypes were mainly concentrated in 25–54 years of age and started to greatly fall after 54 years old. We found that HPV 16 had the highest proportion in all age groups except the ≥45–<55 age group, and the type with the highest percentage in the ≥45–<55 age group was HPV 52. In addition, most of the types have the highest proportion in the ≥25–<35 age group, such as HPV 16, 52, 58, 42, 68, 31, 51, 59, 33, 42, 43, 6 and 45. It is of interest that the proportion of HPV 53, 56, 39, 81 and 73 was highest in the ≥45–<55 age group. The LR-HPV genotype with the highest proportion was HPV 42 in each age group except group T7 (age≥75), of note that HPV 42 showed particular trends, including significant increases in the ≥25–<35 and ≥45–<55 age groups.

Distribution of HPV genotypes in different age groups among positive females. (A) The proportion of HR-HPV genotypes and other possibly carcinogenic types in seven age groups. (B) The proportion of LR-HPV genotypes in seven age groups. APC, annual percentage change; HPV, human papillomavirus. HR-HPV, high-risk human papillomavirus; LR-HPV, low-risk human papillomavirus.
The impact of COVID-19 on HPV infection rate in different pandemic years
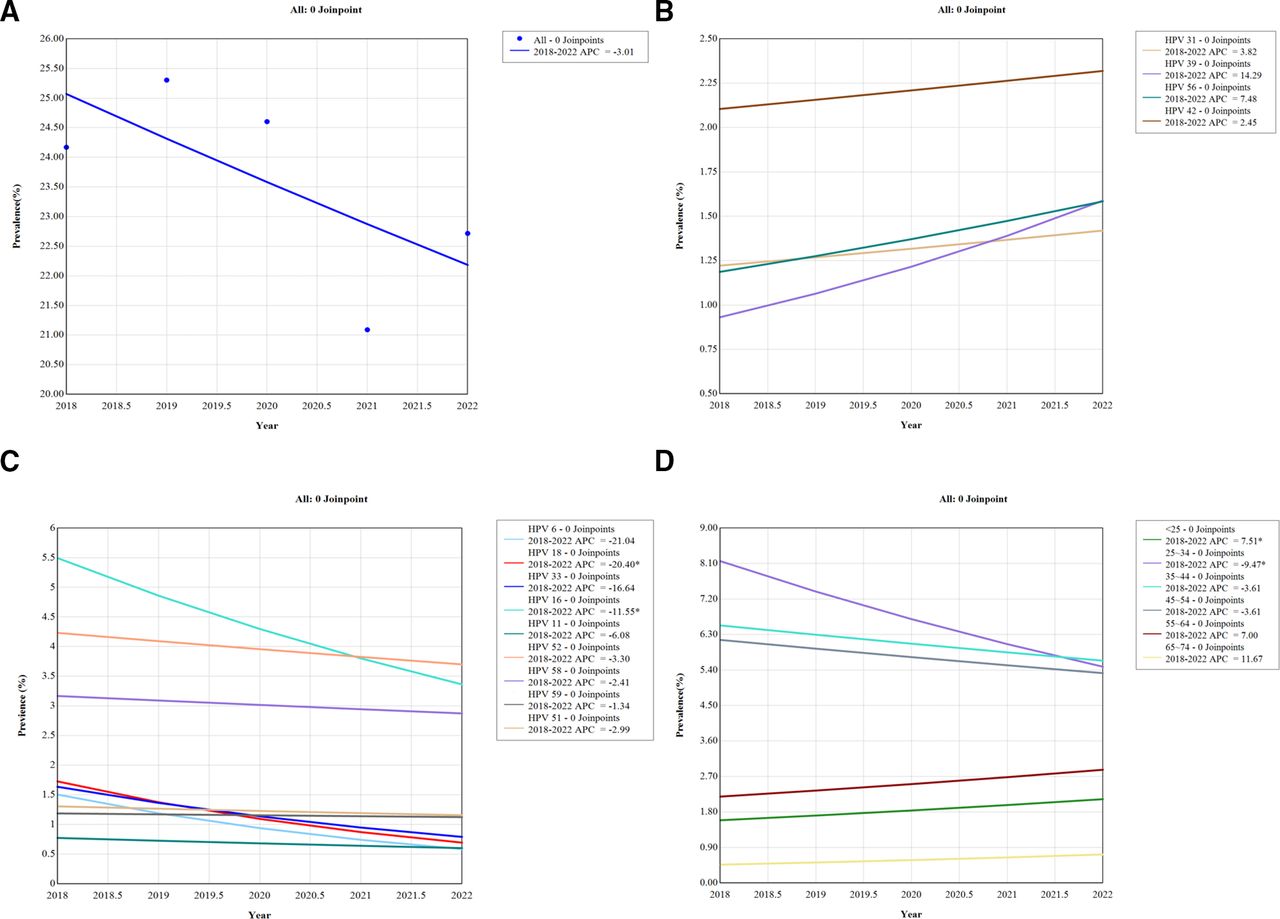
The annual prevalence of HPV infection from 2018 to 2022 was 24.17%, 25.30%, 24.60%, 21.09% and 22.72%, respectively, which have a significant decrease during the second (2021) and third (2022) years of the COVID-19 pandemic. The HPV infection rate was shown significantly different during these 5 years (p<0.001) (table 1). The number of HPV samples received in 2020, 2021 and 2022 reduced by 24.03%, 14.79% and 24.76%, respectively, compared with 2019, the year before the COVID-19 breakout. Moreover, as shown in table 1, the single and double infection rates throughout these 5 years were statistically significant (p<0.05), but the prevalence of triple, quadruple and others greater than or equal to quintuple have no significant difference with the p>0.05. In addition, using Joinpoint time trend analysis, the annual percentage change (APC) was −3.01 (95% CI: −8.90 to −3.26, p=0.218) from 2018 to 2022. The trend was not statistically significant in 2018–2022 (figure 4A).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trends of prevalence of HPV infection in Weifang from 2018 to 2022. (A) Total prevalence of HPV infection; (B) increased HPV genotype; (C) decreased HPV genotype; (D) different age groups HPV infection. *Indicates that the APC is significantly different from zero at the alpha=0.05 level (p<0.05). APC, annual percentage change; HPV, human papillomavirus.
Trends of the prevalence of type-specific HPV infection, and the infection across age groups
Trends in the prevalence of type-specific HPV infection were assessed by year. The prevalence of HPV 39 (APC, 14.29; 95% CI: −5.75 to 38.59, p=0.115), HPV 56 (APC, 7.48; 95% CI: −7.96 to 25.54, p=0.236), HPV 31 (APC, 3.82; 95% CI: −3.19 to 11.33, p=0.187) and HPV 42 (APC, 2.45; 95% CI: −9.41 to 15.87, p=0.575) increased over 2018–2022 (figure 4B). The prevalence of HPV 16 (APC, −11.55; 95% CI: −18.81 to −3.74, p<0.05), HPV 18 (APC, −20.40; 95% CI: −32.41 to −6.25, p<0.05), HPV 6 (APC, −21.04; 95% CI: −38.76 to 1.81, p=0.059), HPV 33 (APC, −16.64; 95% CI: −31.57 to 1.50, p=0.06), HPV 11, 52, 58, 59 and 51 decreased over 2018–2022 (figure 4C). Infections with each genotype from 2018 to 2022 are summarised in online supplemental table S2 and significant differences in distribution were seen for HPV types 16, 52, 53, 68, 56, 66, 39, 33, 18, 73, 43, 6 and 11 during this period (p<0.05).
The age distribution of HPV prevalence in 5 years was also counted in online supplemental table S3, with age groups T2, T3, T4 and T5 displaying significant differences in annual HPV-positive participants, which ranged in age from 25 to 55 (p<0.05). The annual prevalence of HPV infection of the <25 years group (APC, 7.51; 95% CI: 1.96 to 13.35, p<0.05), ≥55–<65 years old group (APC, 7.0; 95% CI: −5.51 to 21.16, p=0.181) and ≥65–<75 years group (APC, 11.67; 95% CI: −4.26 to 30.25, p=0.107) increased over 2018–2022 (figure 4D). The annual prevalence of HPV infection in the ≥25–<35 years group (APC, −9.47; 95% CI: −15.07 to −3.48, p<0.05), ≥35–<45 years group (APC, −3.61; 95% CI: −10.30 to 3.57, p=0.202) and ≥45–<55 years group (APC, −3.61; 95% CI: −10.33 to 3.62, p=0.204) decreased over 2018–2022 (figure 4D).
Discussion
This study assessed the overall HPV infection rate, which was discovered to be 23.64% (8998/38 056). Notably, there were significant variations in the prevalence of HPV among different cities in Shandong province, China. For instance, in Weihai city,15 the HPV infection prevalence was 9.61% among 4601 women who were included in the study from April 2007 to March 2010. In Qingdao city,16 the HPV infection rate was found to be 32.2% (1459/4534) among the enrolled samples during the period of November 2011 to October 2014. The prevalence of HPV infection in Jinan was found to be 25.3% (2651/10 306)17 based on data collected from January to December of 2012. Additionally, the overall HPV infection rate in Shandong province was 28.4% (26 839/94 489),18 according to HPV analyst data gathered between January 2011 and June 2017. In this study, the infection rates of several genotypes were significantly different from other previous publications with a large sample size in Shandong province,15–18 especially for HPV 16, 52, 18 and 6. These above-mentioned statistical findings were obtained between 2007 and 2017, when HPV vaccines were not widely available in Shandong province. Since HPV vaccines have been available early in some European countries, research have shown that these vaccines dramatically reduce HPV infection among young women,19 and significantly reduce the incidence of cervical cancer in young women.20 However, in China, the HPV vaccination rate is reported to be only about 5.5%, so it is urgent to advance the HPV immunisation programme. In addition, the difference in economic conditions, cultural habits, sampling periods and lifestyles may contribute to the variable HPV prevalence between different cities in China.17 21 22 This study reports the genotype data of HPV infection from a large number of females in Weifang city for the first time, during the period of 2018 to 2022 after three HPV vaccines were all listed in China, which provides data basis for future studies on the epidemiological characteristics of HPV infection after vaccination among the local population in Weifang.
HPV infection, particularly persistent HR-HPV infection, is a major risk factor for precancerous lesions and cervical cancer. HPV 16 and HPV 18 are responsible for over 70% of cervical cancers globally.2 According to one study that pooled data from nine countries, HPV 16, 18, 45, 31, 33, 52, 58 and 35 were the most prevalent HPV types in patients with cervical disease, whereas types 16, 18, 45, 31, 6, 58, 35 and 33 were the most common in control women (without cervical cancer).2 According to the other study, women with normal cytology were most likely to be infected with HPV types 16, 18, 31, 58, 52 and 33.23 In this study, HPV 16 was found to be the most prevalent HR-HPV genotype, followed by HPV 52, 58, 53 and 68. In contrast, HR-HPV 18 was not a common infection type in this study, with an infection rate of 1.17%, which is in line with the findings of a study conducted in 37 cities in China.17 The first three HPV genotypes (16, 52 and 58) were consistent with previous research of Shandong province,18 Human province22 and Hangzhou city,24 but in some other Chinese cities, such as Wuhan,25 Jiangsu,26 Beijing27 and Shanghai,28 the three most common HPV genotypes were HPV 52, 16 and 58, indicating that there are some differences in the prevalence of HPV genotype throughout China. One study suggested that HPV 52 infections are more common among healthy individuals, and HPV 58 has been linked to cervical cancer.29 In this study, HR-HPV 52 and 58 were found to be most prevalent in the age groups T2, T3 and T4, with ages ranging from 25 to 54 years old. On 30 August 2022, the National Medical Products Administration in China approved expanding the immunisation age for the nonavalent HPV vaccine from 16–26 years to 9–45 years. The prevalence of 52 and 58 types may be somewhat decreased by widening the age of vaccination with the nonavalent vaccine. Because, vaccine effectiveness will predominantly depend on the extent of previous infection and type-specific HPV prevalence in the population cohort vaccinated.30
LR-HPVs have been associated with anogenital malignancies.31 Previous studies have reported that 81 or 6 were the most common LR-HPV genotypes.17 25 26 28 However, this study reveals that LR-HPV 42 has the highest infection rate across most age groups, which differs from the prevalence of LR-HPV types in other regions of China. As shown in online supplemental table S4, this study presents novel finding that HPV 42 has the highest infection rate among LR-HPV, which is being reported for the first time. Recent research suggests that HPV 42 recapitulates the molecular hallmarks of oncogenic.31 Furthermore, a case report has documented cervix seborrheic keratinoid lesions associated with HPV 42,32 and a study has confirmed the association of HPV 42 with tumour cells of digital papillary adenocarcinoma.33 Although HPV 42 is one of the most susceptible LR-HPV genotypes in Chinese population, there have been limited studies focused on the prevalence of HPV 42, which is worthy of attention for further attention and investigation.
Numerous domestic and international research reports have shown that young women had the highest HPV prevalence as the first peak and the second peak occurs in older women, which forms a bimodal pattern of HPV prevalence among different age groups,34 but the age in which the second peak occurs varies.12 17 21 25 28 In addition, the ‘two-peak pattern’ is not common in other studies in China.16 26 In this study, we found that young women under the age of 25 had the highest HPV infection rate (36.74%) with a significant peak, which was in line with previous studies (33.11% within <21 age group),35 and it is lower than overall Shandong province (56% within ≤20 age group),18 Zhejiang province (51.2% within ≤20 group),21 perhaps due to the data were collected from various locations, ages and times. In addition, although there was a slight increase in the prevalence of HPV infection in the ≥35–<45 and ≥55–<65 age groups, no conclusion can be drawn about a second peak of age-specific infection. Young women, who are sexually active after the first sexual encounter and unsensitised immune systems are at risk for HPV infections. However, HPV infection is temporary in most young women and is eliminated by the body as their age increases,36 therefore, the HPV infection rate gradually declines after the age of 20. But a small number of persistent HR-HPV infections can result in cervical cancer if the immune system fails to clear the virus.37 The slight increase in overall infection rate in older women, as well as the increased proportion of older women with multiple infections of double, triple or more genotypes might reflect an impaired immune response caused by hormonal changes at menopause.
The annual prevalence of Weifang fluctuated between 21.09% and 25.30%, decreasing from 2018 to 2022, with a significant decrease in 2021 and 2022. Furthermore, the prevalence among age groups 25–34, 35–44 and 45–54 exhibited an overall decreasing trend from 2018 to 2022. Notably, the infection rate of HPV genotypes 16, 52, 53, 68, 18, 33, 64, 44 and 6 also declined in 2021. This decline may be attributed to the following reasons: first, the continued outbreak of COVID-19 resulted in a decrease in patients or epidemic prevention isolation measures reducing unnecessary sexual activity. Second, the coverage of HPV vaccination in previous years may have a protective effect after 2020, particularly among middle-aged women. Over the course of 5 years, significant changes in the prevalence of certain genotypes have been observed. While some genotypes have shown decreasing infection rates, HPV 56, 39, 31 and 42 have exhibited an increasing trend, with a higher infection rate in 2022 compared with the previous 4 years. For future studies, we will continue to collect data and track the trend of HPV prevalence and different genotypes over the coming years, which is of great significance for the early prevention and treatment of cervical cancer in this region.
In summary, this study described the prevalence characteristics of HPV among women in Weifang with a large sample size over a 5 year period. There were some limitations. First, we were unable to determine whether these patients were vaccinated for HPV. HPV vaccination has a significant impact on HPV test results. Second, we have only listed the possible reasons for the decrease in HPV infection during the pandemic, without detailed research studies, then we will consider this in future studies. Third, the distribution of HPV infection genotypes cannot be correlated with different cervical abnormalities due to the lack of cervical cytological or histological findings.
Conclusions
This study revealed that the overall HPV prevalence was high (23.64%) in Weifang city between 2018 and 2022, and women aged less than 25 years showed the highest HPV prevalence. HPV 16, 52 and 58 were the three most common HR-HPV genotypes, which were mainly in accordance with the present situation of HPV prevalence in China. Importantly, HPV 42 was first reported to have the highest positive rate in LR-HPV types. The data from this study may serve as a baseline for further monitoring of HPV genotype distribution and will provide guidance and increase the accuracy of future local HPV vaccination strategies.
Data availability statement
Data are available on reasonable request. The data sets used and/or analysed during this study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The epidemiological study has been approved by the Affiliated Hospital of Weifang Medical University, Weifang Medical University (wyfy-2022-ky-018). Participants gave informed consent to participate in the study before taking part. All methods were carried out in accordance with the relevant guidelines and regulations.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ML performed the statistical analysis and wrote this manuscript. XZ and LG participated in the design of the study. WS and XJ performed the sample and data collection. Guarantor: ML. All authors reviewed the manuscript.
Funding This work is supported by Start-up Funds for Doctoral Research Projects of Affiliated Hospital of Weifang Medical University (2021BKQD4) and the Natural Science Foundation of Shandong Province, China (ZR2023QH061).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.