Article Text

Abstract
Objectives This study was conducted to evaluate the ability of risk assessment to predict healthcare resource utilisation (HCRU), costs, treatments, health-related quality of life (HRQoL) and survival in patients diagnosed with chronic thromboembolic pulmonary hypertension (CTEPH).
Design Retrospective observational study.
Setting Pulmonary hypertension referral centre in the UK.
Participants Adults diagnosed with CTEPH between 1 January 2012 and 30 June 2019 were included. Cohorts were retrospectively defined for operated patients (received pulmonary endarterectomy (PEA)) and not operated; further subgroups were defined based on risk score (low, intermediate or high risk for 1-year mortality) at diagnosis.
Primary and secondary outcome measures Demographics, clinical characteristics, comorbidities, treatment patterns, HRQoL, HCRU, costs and survival outcomes were analysed.
Results Overall, 683 patients were analysed (268 (39%) operated; 415 (61%) not operated). Most patients in the operated and not-operated cohorts were intermediate risk (63%; 53%) or high risk (23%; 31%) at diagnosis. Intermediate-risk and high-risk patients had higher HCRU and costs than low-risk patients. Outpatient and accident and emergency visits were lower postdiagnosis for both cohorts and all risk groups versus prediagnosis. HRQoL scores noticeably improved in the operated cohort post-PEA, and less so in the not-operated cohort at 6–18 months postdiagnosis. Survival at 5 years was 83% (operated) and 49% (not operated) and was lower for intermediate-risk and high-risk patients compared with low-risk patients.
Conclusions Findings from this study support that risk assessment at diagnosis is prognostic for mortality in patients with CTEPH. Low-risk patients have better survival and HRQoL and lower HCRU and costs compared with intermediate-risk and high-risk patients.
- Quality of Life
- Mortality
- Chronic airways disease
Data availability statement
No data are available. The data in this study will not be made publicly available as they were obtained from NHS Digital by the researchers under a data sharing agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Using a rigorous methodology, we have linked two databases to provide a real-world evidence profile of a large cohort of patients treated for chronic thromboembolic pulmonary hypertension (CTEPH).
Our study supports the use of a risk stratification approach used in pulmonary arterial hypertension in a large cohort of patients with CTEPH, demonstrating differences in survival in the three risk bands at diagnosis.
This study adds to a limited literature describing the economic burden of CTEPH, with data available prediagnosis and postdiagnosis and by risk status at diagnosis.
The duration of follow-up precluded meaningful comparisons regarding the long-term economic impact of pulmonary endarterectomy (PEA) surgery compared with other treatment approaches.
Although results of the risk assessment analysis are reported separately by PEA status (ie, operated vs not operated), it was not feasible to adjust the analysis for differences in baseline variables between the operated and not-operated cohorts.
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is characterised by obstruction of the pulmonary arteries and is frequently associated with a small-vessel vasculopathy.1 It is caused by non-resolution of pulmonary thromboembolic disease, although some patients have no history of previous venous thromboembolism.1–5 When left untreated, mortality is higher in CTEPH than in many common cancers.5
Based on registry data from European healthcare systems, the estimated annual incidence of CTEPH is 3–6 cases per 1 000 000 population,2 6 and the estimated 2-year cumulative incidence after pulmonary embolism (PE) is 2.3%.7 CTEPH is challenging to diagnose due to non-specific initial symptoms and patients often present at an advanced stage,2 4 by which time health-related quality of life (HRQoL) is already substantially impaired.8
A multimodal approach is increasingly being used to treat CTEPH, including pulmonary endarterectomy (PEA), percutaneous balloon pulmonary angioplasty (BPA) and drug therapies.3 5 Patients with CTEPH who are candidates for surgery can experience substantial symptom relief and a marked improvement in haemodynamics after PEA,2 9 which offers the best prospect of improved long-term outcomes, including survival.10 For patients ineligible for surgery, BPA can improve pulmonary haemodynamics, 6 min walk distance and WHO functional class (FC).5 11 For the treatment of CTEPH in patients with distal disease or residual PH post-PEA, riociguat, an oral soluble guanylate cyclase stimulator, and treprostinil, a subcutaneous prostacyclin analogue, are approved by the European Medicines Agency.3 12–14 Pulmonary arterial hypertension (PAH)-targeted therapies, such as phosphodiesterase type 5 inhibitors (PDE-5i) and endothelin receptor antagonists (ERA), are also often used off-label for treating CTEPH.15 16 In the UK, patients with both operable and inoperable CTEPH are eligible for treatment with PDE-5i, ERA and prostanoids, whereas riociguat is commissioned only for patients with inoperable disease and residual PH post-PEA.17
Over the last decade, recognition of the importance of assessing prognosis in patients with PAH has grown.18 Categorising patients as at low, intermediate or high risk of 1-year mortality at diagnosis is used to guide initial treatment decisions. Regular assessments are recommended to improve morbidity and mortality by reaching low-risk status.2 19–22 In CTEPH, risk assessment is less established. The 2015 European Society of Cardiology (ESC) and European Respiratory Society (ERS) risk assessment tool to predict 1-year mortality in patients with PAH2 has been investigated in CTEPH within COMPERA (Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension) and SPAHR (Swedish PAH Registry).10 23 24
This retrospective observational study was conducted to generate real-world evidence (RWE) from a high-volume PH referral centre on the demographic and clinical characteristics, treatment patterns, economic burden, HRQoL and overall survival (OS) for patients diagnosed with CTEPH. Second, we sought to compare these characteristics prediagnosis and postdiagnosis based on operated (PEA) status and 1-year risk of mortality at diagnosis.
Methods
Data sources
Data were collected from the electronic medical record database used at the Sheffield Pulmonary Vascular Disease Unit (SPVDU) based at Royal Hallamshire Hospital and linked with data from the National Health Service (NHS) Hospital Episode Statistics (HES) database, as previously described.25 26 The SPVDU is a nationally commissioned PH referral centre covering a population of approximately 15–20 million.27
The SPVDU database contains clinical management and demographic data for all referred patients, including confirmed diagnoses, diagnostic procedures, clinical tests, treatment prescribed and specialist consultations. Missing data on reasons for not operating were supplemented by manual searching and reviewing of clinical records for each patient in the not-operated cohort. The HES database contains details on patient comorbidities, hospital admissions, accident and emergency (A&E) visits and outpatient consultations at all NHS England hospitals.28
Aggregated, pseudoanonymised data were used in this study. HES data were linked by NHS number and date of birth to SPVDU data before being deidentified and made accessible for analysis in this study. Death data in the SPVDU database were captured through linkage to NHS death records.
Categories with <7 patients in tables have been masked in line with data protection requirements to ensure that patient confidentiality was maintained.29 Where only a single count was masked as ‘<7’, and therefore, could be further identified, the category with the next lowest number was also suppressed to avoid calculation of the small value. No data were excluded from the analyses due to suppression. Kaplan-Meier (KM) curves were cut when the number at risk dropped to <10% of the stratum size.30
Study design
Adult patients (≥18 years old at diagnosis) with a diagnosis of CTEPH (mean pulmonary artery pressure ≥25 mm Hg and persistent perfusion defects following at least 3 months of anticoagulation and other causes of PH excluded) were included in this retrospective observational cohort study if they were diagnosed with CTEPH between 1 January 2012 and 30 June 2019 and had ≥90 days of follow-up in the SPVDU database. No minimum follow-up or look-back time for the HES was required.
For the analyses, patients were categorised as operated (defined as having received PEA surgery after diagnosis and within the study period) or not operated (no PEA surgery during the study period). The annual incidence of new CTEPH diagnoses was calculated based on the referral population.27 31
For all study participants, the study index date was defined as the first CTEPH diagnosis date within the study period. The date of PEA was defined as a secondary index date in the operated cohort for additional survival analyses. Patients were followed from diagnosis until date of death or last contact, or end of study observation (30 September 2019).
Risk categorisation
The Kylhammar et al risk-assessment tool was adapted to categorise patients at diagnosis as being at low, intermediate or high risk of 1-year mortality (online supplemental information).32 The Kylhammar tool is based on the 2015 ESC/ERS risk-assessment framework and has been used previously in patients with PAH from the SPAHR.32 The composite risk score used measurements at diagnosis for six clinical variables: WHO FC, incremental shuttle walk test (ISWT), right atrial pressure, cardiac index, mixed venous oxygen saturation and right ventricular ejection fraction as assessed by cardiac magnetic resonance.33 Previously published thresholds for the ISWT were used.33–35 Each variable was graded from 1 to 3 (1=low risk, 2=intermediate risk and 3=high risk). A mean grade was calculated and rounded to the nearest integer to determine the risk group.32 WHO FC and ISWT were required as a minimum to calculate a risk score. If either was unavailable, the score was labelled ‘missing/undetermined’.
Supplemental material
Study measures
Variables and outcomes collected from the SPVDU database included patient demographics and clinical characteristics; treatments prescribed at or within the 90 days following diagnosis; 1-year, 3-year and 5-year survival after diagnosis; and changes in HRQoL. HRQoL was measured using the EmPHasis-10, a PH-specific questionnaire. Scores range from 0 to 50, with higher scores indicative of worse HRQoL.36 37 In the operated cohort, HRQoL was assessed within 90 days of diagnosis but prior to PEA surgery, and 6–18 months post-PEA. In the not-operated cohort, the assessments were within 90 days of diagnosis and 6–18 months postdiagnosis.
Variables and outcomes collected from the HES database included: comorbidities in the 5 years prior to diagnosis; 1-year, 3-year and 5-year survival after diagnosis; healthcare resource utilisation (HCRU) 1-year, 2-year and 3-year prediagnosis and 1-year, 3-year and 5-year postdiagnosis; and costs for patients who had 1 and 3 years of follow-up data in HES. Inpatient hospitalisations were categorised as either longer than 1 day or ‘same-day visits’, meaning the admission and discharge date was the same. Outpatient visits were defined as any activity occurring in hospital under an outpatient setting.
Statistical analysis
This study was descriptive, without predefined hypotheses. Although results for the operated and not-operated cohorts are reported, no direct comparison between these cohorts was undertaken. Categorical variables are reported as frequency (n) and percentage (%). Continuous variables are reported as median (Q1, Q3) and mean (±SD). OS was evaluated with KM estimates, with follow-up time starting from index date and censoring at date of last contact. Costs are described using national average tariff prices in England for 2019.38
Patient and public involvement
Patients were not involved in the conception, design or conduct of this retrospective research.
Results
A total of 683 patients were diagnosed with CTEPH between January 2012 and June 2019. Based on a referral population of 15–20 million, the annual incidence of CTEPH was 4.6–6.1.27 31 The median period from first record in HES to diagnosis at SPVDU was 4.3 years (figure 1). The median follow-up time from diagnosis to study exit was 2.2 years in SPVDU and 2.5 years in HES. Overall, 193 (28%) patients died during the study period.

Overview of observation times and database coverage in the study. Purple boxes represent HES database; green boxes represent Sheffield PVDU database. EMR, electronic medical record; HCRU, healthcare resource utilisation; HES, Hospital Episode Statistics; HRQoL, health-related quality of life; PEA, pulmonary endarterectomy; PVDU, Pulmonary Vascular Disease Unit.
Demographics and clinical characteristics
Patient demographics and clinical characteristics at diagnosis are presented in table 1. Overall, 285 (42%) patients received PEA prior to 30 September 2019; 398 (58%) were not operated. At the time of the analysis, not all patients with operable disease had undergone PEA, and therefore, 268 (39%) patients were included in the operated cohort and 415 (61%) in the not-operated cohort. In a post hoc data check using clinical records, the major reasons for not operating were identified in 398 not-operated patients as follows: 91 (23%) declined PEA; 69 (17%) had surgically inaccessible disease; 133 (33%) were medically inoperable (due to comorbidities); 47 (12%) had disease that was considered too mild by the surgical team to benefit from intervention and 24 (6%) were awaiting PEA. For the remaining patients, reasons for not operating were missing or unclear (n=34 (9%)).
Demographics and clinical characteristics at diagnosis of patients with CTEPH
Median age at diagnosis was 67 years. Median time from diagnosis to PEA in the operated cohort was 8.6 months. Haemodynamic values were largely similar between the two cohorts. Most patients in both cohorts were assessed as intermediate risk or high risk at diagnosis.
Comorbidities identified prior to diagnosis
PE was the most commonly reported comorbidity (74%) in both cohorts (figure 2). Hypertension, chronic obstructive pulmonary disease, other obstructive lung disease, heart failure, ischaemic heart disease and valvular heart disease were reported in >25% of not-operated patients. Hypertension was reported in >25% of operated patients.

Comorbidities recorded as present in the 5 years prior to CTEPH diagnosis. Data were collected from the HES database. CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CTEPH, chronic thromboembolic pulmonary hypertension; HES, Hospital Episode Statistics.
Treatment prescribed at diagnosis
Most patients were prescribed PAH-specific therapies at or within 90 days following diagnosis: 74% (197/267) of operated patients and 75% (306/410) of not-operated patients. PDE-5i monotherapy was most commonly prescribed in 96% (190/197) of operated and 92% (280/306) of not-operated patients, respectively. Among low-risk, intermediate-risk and high-risk groups, treatment was prescribed in 33%, 75% and 87% of operated patients and in 34%, 72% and 90% of not-operated patients.
HCRU and costs
Inpatient hospitalisations, same-day visits and outpatient consultations were similar between operated and not-operated patients at prediagnosis and postdiagnosis (figure 3 and online supplemental table 1). Outpatient consultations among operated patients 1-year postdiagnosis decreased compared with 1-year prediagnosis; this measure also decreased in not-operated patients. A&E visits fell to 0 in both cohorts after diagnosis. Among patients who had inpatient hospitalisations during the first year postdiagnosis, median (Q1, Q3) duration was 8.7 (6.0, 12.0) days in the operated cohort and 3.0 (2.0, 8.0) days in the not-operated cohort.

Median HCRU per patient per year, 1 year before and 1 and 3 years after CTEPH diagnosis in (A) operated patients and (B) not-operated patients. *HCRU at 3 years postdiagnosis represents median per year over 3 years, not during the third year. Same-day visits defined as inpatient visit where admission and discharge date are the same. A&E, accident and emergency; HCRU, healthcare resource utilisation.
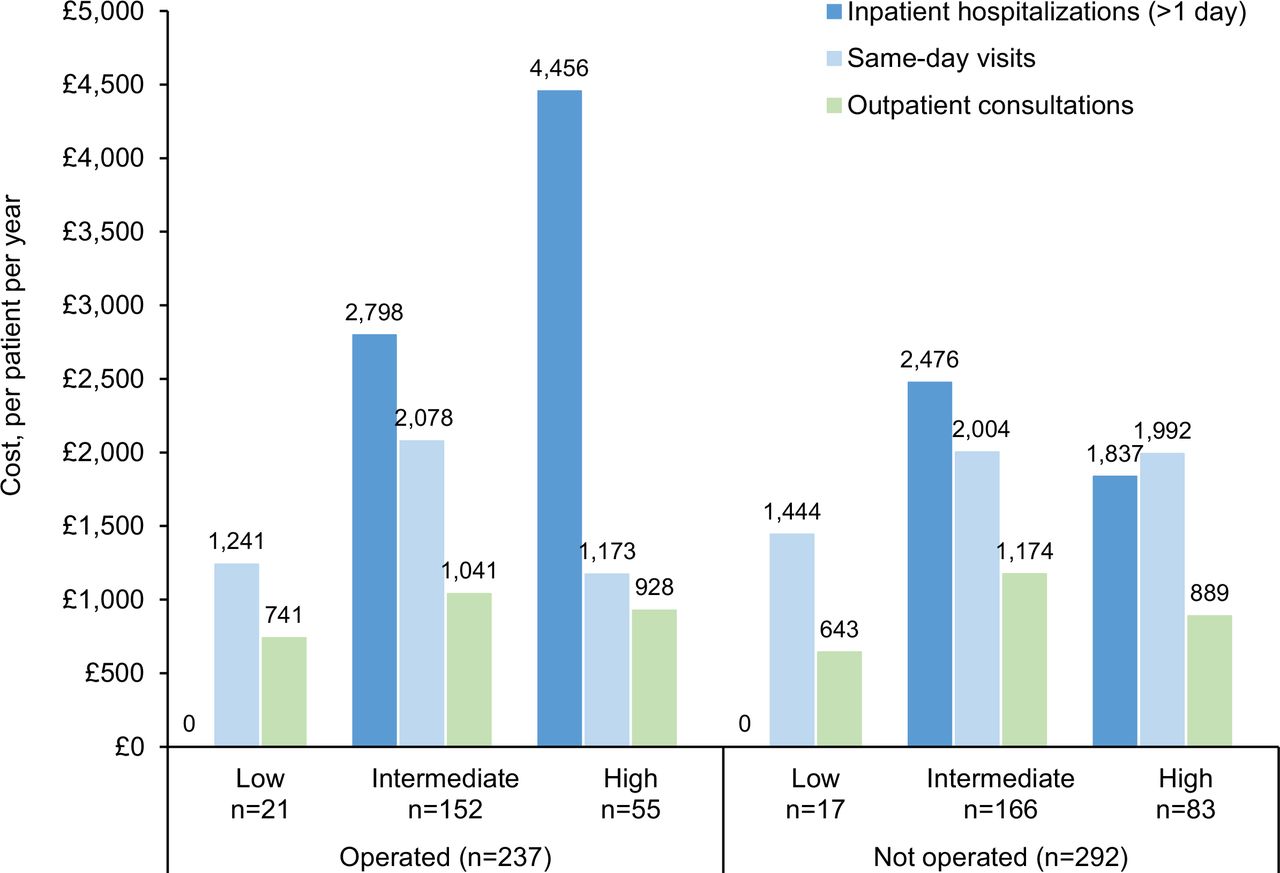
Intermediate-risk and high-risk patients had higher HCRU than low-risk patients (figure 4). In both cohorts, outpatient and A&E visits were lower postdiagnosis for all risk groups versus prediagnosis. In the first year following diagnosis, high-risk patients in the operated cohort had the highest costs, due to inpatient hospitalisations (figure 5). Across risk groups in both cohorts, costs for inpatient hospitalisations were the most variable while costs for same-day visits and outpatient consultations were similar.

Median HCRU per patient in the year before and after CTEPH diagnosis, stratified by risk category at diagnosis in (A) operated and (B) not-operated patients. Same-day visits defined as inpatient visit where admission and discharge date are the same. A&E, accident and emergency; HCRU, healthcare resource utilisation.

Median cost (GBP) per patient in the year after CTEPH diagnosis. Costs were obtained from HES, which is for administrative use; therefore, practices might vary across hospitals/clinical coders. Costs associated with PEA surgery in patients with CTEPH are reimbursed separately and the values quoted for cost of care do not include those associated with PEA surgery. Same-day visits defined as inpatient visit where admission and discharge date are the same. CTEPH, chronic thromboembolic pulmonary hypertension; GBP, British Pound Sterling; HES, Hospital Episode Statistics; PEA, pulmonary endarterectomy.
Health-related quality of life
Paired analysis of median EmPHasis-10 scores at diagnosis and follow-up by cohort and risk group are shown in figure 6. Overall, there was a median (Q1, Q3) decline (improvement) from diagnosis to follow-up of 10 (19, 1) in the operated cohort and 2 (8, 3) in the not-operated cohort. Intermediate-risk and high-risk patients in the operated cohort showed a median decline of 10.5 (20.5, 0.5) and 14 (19, 1), respectively, at follow-up, while in the not-operated cohort, median declines were 2 (7, 3) and 3 (9, 3). Due to data suppression rules, paired analysis of low-risk patients could not be conducted. At diagnosis, median EmPHasis-10 score was 18 for all low-risk patients, 20 for operated low-risk patients and 13 for not-operated low-risk patients.

Median EmPHasis-10 scores at diagnosis and follow-up in the (A) operated cohort and (B) not-operated cohort by risk score at diagnosis. Due to suppression rules, paired analysis of low-risk patients could not be conducted. The EmPHasis-10 is a quality-of-life instrument developed and validated specifically for assessment of HRQoL in patients with PH.36 37 Higher scores are indicative of worse HRQoL.37 HRQoL, health-related quality of life; PEA, pulmonary endarterectomy; PH, pulmonary hypertension; Supp, suppressed.
Overall survival
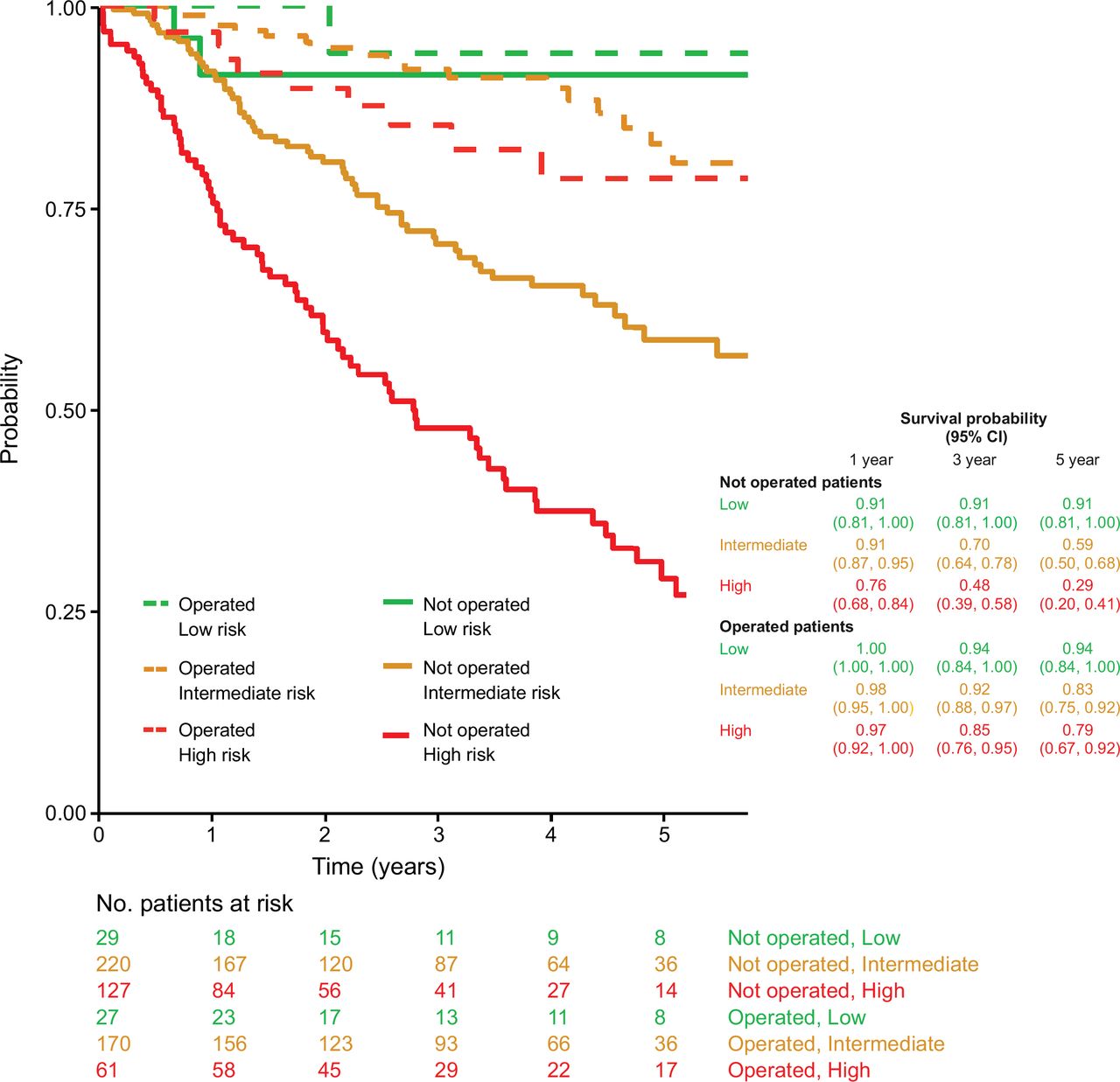
The probability of survival at 1, 3 and 5 years was 98%, 91% and 83%, respectively, in the operated cohort and 85%, 63% and 49%, respectively, in the not-operated cohort. When stratified by risk category at diagnosis, survival was lower for intermediate-risk and high-risk patients versus low-risk patients (figure 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival from diagnosis in the operated and not-operated cohorts by risk score at diagnosis. Solid lines represent the not-operated cohort and dashed lines represent the operated cohort.
Discussion
This retrospective study has evaluated real-world HCRU, costs, HRQoL and survival data from a European PH referral centre for patients diagnosed with CTEPH, stratified by operated status and risk score at diagnosis. To our knowledge, this is the first study to analyse economic burden and HRQoL for CTEPH by risk stratification.
Risk assessment, with the aim of guiding treatment decisions, is not yet established in CTEPH. Our risk stratification method was based on the risk-assessment tool developed for PAH32 and consistent with previous studies in patients with CTEPH that used the ESC/ERS 2015 framework, showing most patients are at intermediate or high risk at diagnosis.10 39 More notably, our study supports the finding that CTEPH patients stratified by risk at diagnosis show considerable differences in survival.10 23 39 Using CTEPH data on not-operated patients from the COMPERA registry, for example, Delcroix et al estimated 1-year and 5-year survival rates at 76% and 33% for high-risk patients and 99% and 88% for low-risk patients; by comparison, rates in this study in the not-operated cohort were 76% and 29% for high-risk patients and 91% at both time points for low-risk patients.39 Sandqvist et al compared survival among operated and not-operated patients who were diagnosed with CTEPH between 2008 and 2016 and found significant differences (p<0.001). Survival at 1, 3 and 5 years stratified by risk assessment at diagnosis was 100%, 98% and 82%, respectively, in the low-risk group; 93%, 81% and 71%, respectively, in the intermediate-risk group; and 75%, 48% and 38%, respectively, in the high-risk group.10 While these rates for low-risk and intermediate-risk patients are similar to our study (in both the operated and not-operated cohorts), high-risk patients in the operated cohort of our study had notably better survival (97%, 85% and 79% at 1, 3 and 5 years, respectively). In the Sandqvist et al study, 32% of patients underwent PEA; in these patients, survival was 96%, 92% and 88% at 1, 3 and 5 years, which is more comparable to our study.10
There are few studies reporting on the HCRU and costs of care for patients with CTEPH, and none that are recent or include risk stratification. For both operated and not-operated patients in this study, the pattern of HCRU remained similar prediagnosis and postdiagnosis. The exceptions were A&E visits, which decreased following a CTEPH diagnosis, regardless of surgery and outpatient consultations, which noticeably decreased postdiagnosis in the operated cohort. This finding may reflect the impact of confirming a diagnosis of CTEPH and establishing a treatment regimen. Analysing HCRU by risk showed no major differences in the operated cohort, with the exception of prediagnosis A&E visits for low-risk patients compared with intermediate-risk and high-risk patients. In the not-operated cohort, low-risk patients had notably lower HCRU (eg, no inpatient hospitalisations before or after diagnosis). It seems that routine, preplanned follow-up helps prevent A&E visits and unplanned hospitalisation postdiagnosis, an important consideration for healthcare systems.
A retrospective chart review of 119 patients from 6 European countries who were diagnosed with CTEPH between 2006 and 2009 reported a median of 1.0 inpatient hospitalisations per patient per year16; this is consistent with our study. Similarly, a previous UK study quantified the median inpatient stay during PEA to 11 days; in this study, operated patients had a median inpatient stay of 8.7 days, which included PEA and was averaged over the first year after diagnosis. HCRU in our study was considerably lower than that reported in a retrospective analysis of a US commercial claims database in 161 patients with CTEPH between 2004 and 2009.40 In this study, mean per-patient-per-year HCRU across all measures was higher than our results, including outpatient visits (11.2 prediagnosis vs 14.0 postdiagnosis), inpatient visits (6.7 prediagnosis vs 23.6 postdiagnosis) and A&E visits (3.0 prediagnosis vs 5.3 postdiagnosis). The increased HCRU after diagnosis also contrasts with our results. These differences may be attributable to advances in and access to medical and surgical therapies for CTEPH patients over time (given the different study periods), and to differences between the UK and US healthcare systems. Our study is also based on clinical data, as opposed to claims data.
Risk category at diagnosis appeared to influence the cost of treatment for both operated and not-operated patients. Costs for inpatient hospitalisations (>1 day and same-day visits) were higher for operated patients and highest among intermediate-risk and high-risk patients. This finding may reflect the cost of PEA for follow-up visits at the surgical centre and management of complications. Both measures fell by 3 years postdiagnosis.
HRQoL was assessed in our study using the patient-reported EmPHasis-10; median scores at diagnosis were 31 for operated and 30 for not-operated patients. A lower average score of 24 was reported in a US study of 30 newly diagnosed patients with CTEPH.36 The higher score in our study is influenced by the proportion of high-risk patients in both cohorts, who reported worse HRQoL at diagnosis than low-risk and intermediate-risk patients. Notably, low-risk not-operated patients in our study reported the lowest score of any group. Although our low-risk groups were small, their better HRQoL may be an important consideration for treatment decision-making.
Several studies have shown that patients undergoing PEA have improved HRQoL following surgery, particularly those with no residual PH, while not-operated, medically treated patients are less likely to experience marked improvements in HRQoL.8 This is supported by our study, where median EmPHasis-10 scores improved dramatically post-PEA but only slightly postdiagnosis in the not-operated cohort. Given that survival was largely unchanged in low-risk operated and not-operated patients compared with intermediate-risk and high-risk patients, it may be reasonable not to perform PEA and closely observe operable patients with a low-risk status and good HRQoL.
In this study, 43% of patients underwent PEA, a similar rate as reported in other publications and the UK National Audit of Pulmonary Hypertension.41 In some international registries, the percentage of patients undergoing PEA is higher, but this likely reflects in part the more selected nature of patients in these registries (which are often dominated by surgical centres), whereas the ASPIRE registry used in this study includes all consecutive patients seen in a PH referral centre. Indeed, the population-based PEA rate for our centre is in the range of 1.9–2.5/million population/year, based on our estimated referral population of 15–20 million and a total of 285 patients operated over 7.5 years. This is similar to the rate of 2.2/million population/year based on data from the UK National Audit between 2010 and 2020,41 and higher than the reported rates of 1.7/million/year in Europe and 0.9/million/year in the USA.42 43 Further work is required to understand factors that underlie therapeutic decision-making for patients with CTEPH, given that surgical intervention in suitable patients is associated with improved survival.43
This study has a number of limitations. Sample size limitations made it infeasible to stratify the risk assessment analysis by PEA status (ie, operated vs not operated). Some analyses were limited due to a lack of follow-up data at 1 and 3 years. Due to small patient numbers within subgroups by risk category, data suppression was applied to comply with data privacy rules, although this did not prevent interpretation of planned measures. Missing data were completed in a post hoc analysis of clinical records, showing 17 (4%) patients who had PEA but were not included in the operated cohort due to data availability at extraction, and 7 (2%) who were categorised as not having CTEPH. Due to the small numbers, inclusion of these misclassified patients in the analysis is unlikely to have meaningfully impacted the results. Given the limited duration of follow-up we were unable to make meaningful comparisons regarding the long-term economic impact of PEA surgery compared with other treatment approaches. In addition, due to the timing of this study, few patients in the UK underwent BPA or received treatment with riociguat.44 Nonetheless, using a rigorous methodology, we linked two databases to provide an RWE profile of patients treated for CTEPH in a large cohort.
Our results confirm that the economic burden of CTEPH is high and that HCRU and costs are higher in intermediate-risk and high-risk patients. Low-risk patients with CTEPH also have better survival and HRQoL, compared with intermediate-risk and high-risk patients. Whether treatment strategies aimed at achieving, where possible, a low-risk profile in patients with CTEPH can improve patient outcomes requires further research. In addition, the diagnosis of CTEPH reduces unplanned HCRU (via A&E visits) among operated and not-operated patients, regardless of risk group, emphasising the importance of achieving a diagnosis and its positive impact on health-seeking behaviour.
Data availability statement
No data are available. The data in this study will not be made publicly available as they were obtained from NHS Digital by the researchers under a data sharing agreement.
Ethics statements
Patient consent for publication
Ethics approval
The reported study was non-interventional, and analysis was based on secondary data. No identifying data were prospectively collected in any of the planned approaches. Ethics approval was obtained from the Research Ethics Committee (REC) of the NHS Health Research Authority and from the Confidentiality Advisory Group (CAG) to secure s251 approval for the linkage of patient identifiable data. Following approval from the REC and CAG, an application was submitted through the NHS Digital Data Access Request Service (DARS) to access the required HES data. This application was reviewed and endorsed by the Independent Group Advising on the Release of Data (IGARD). NHS Digital and the involved entities signed a Data Sharing Agreement (DSA) to secure access to the HES data.
Acknowledgments
Medical writing and editing support were provided by Diana Steinway, Robin Marwick, and W Mark Roberts of Stratenym, funded by Actelion Pharmaceuticals, a Janssen Pharmaceutical Company of Johnson & Johnson. Data wrangling and linkage were performed by James Allsopp, Scientific Computing, Sheffield Teaching Hospitals NHS Foundation Trust, Royal Hallamshire Hospital, Sheffield, UK. HES data were reused with the permission of NHS Digital. Copyright 2023. All rights reserved. ASPIRE Consortium: Robin Condliffe, Charlie Elliot, Abdul Hameed, Athanasios Charalampopoulos, Alex Rothman, AA Roger Thompson, Judith Hurdman, Iain Armstrong, Robert A Lewis, Lisa Watson, Andrew J Swift, Smitha Rajaram, Catherine Billings, Rehan Quadery, and Jim Wild, all at Sheffield Pulmonary Vascular Disease Unit, Sheffield Teaching Hospitals NHS Foundation Trust, Royal Hallamshire Hospital, Sheffield, UK.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators ASPIRE Consortium: Robin Condliffe, Charlie Elliot, Abdul Hameed, Athanasios Charalampopoulos, Alex Rothman, AA Roger Thompson, Judith Hurdman, Iain Armstrong, Robert A Lewis, Lisa Watson, Andrew J Swift, Smitha Rajaram, Catherine Billings, Rehan Quadery, and Jim Wild, all at Sheffield Pulmonary Vascular Disease Unit, Sheffield Teaching Hospitals NHS Foundation Trust, Royal Hallamshire Hospital, Sheffield, UK.
Contributors Study conception: DGK, AL, RM, AB and AM. Study design: DGK, FE, RM, AB, AM and RS. Data acquisition: AL, NH, SW and LR. Data analysis: AL, NH, SW, CD, FE and LR. Data interpretation: AL, DGK, NH, CD, FE, RM, LR, AB, AM, RS and NP. Guarantor: DGK. All authors contributed to drafting the work and revising it critically for important intellectual content. All authors gave final approval of the version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The authors confirm that GPP3 guidelines were followed throughout the development of the paper.
Funding This study was sponsored by Actelion Pharmaceuticals, a Janssen Pharmaceuticals Company of Johnson & Johnson.
Competing interests DGK has received grants from Janssen Pharmaceuticals and Ferrer; consulting fees from Janssen Pharmaceuticals, MSD, Ferrer, Altavant and United Therapeutics; honoraria from Janssen Pharmaceuticals, MSD, Ferrer and United Therapeutics; funding from Janssen Pharmaceuticals, MSD and Ferrer to attend scientific meetings; has participated in a data safety monitoring board or Advisory Board for Janssen Pharmaceuticals and MSD; serves on the Specialist Respiratory Clinical Reference Group (unpaid) and as the UK National Audit Chair. NH has received honoraria payments from Janssen Pharmaceuticals, Vifor Pharmaceuticals and MSD. SW has received grants from Janssen Pharmaceuticals in support of the current study. CD has received a grant from Janssen, UK for investigator-led research unrelated to the present research, and a speaker’s honorarium from Janssen for an educational lecture. FE, LR and RM have no conflicts to disclose. AB, AM, RS and NP are employees of Actelion Pharmaceuticals. AB, AM and NP own stock in Johnson & Johnson. AL is supported by a British Heart Foundation Senior Basic Science Research Fellowship (FS/18/52/33808).
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.