Article Text

Abstract
Introduction Lifelong learning is the foundation for professionals to maintain competence and proficiency in several aspects of economy and medicine. Until now, there is no evidence of overconfidence (the belief to be better than others or tested) and clinical tribalism (the belief that one’s own group outperforms others) in the specialty of health economics. We investigated the hypothesis of overconfidence effects and their relation to learning motivation and motivational patterns in healthcare providers regarding healthcare economics.
Methods We conducted a national convenience online survey of 116 healthcare workers recruited from social and personal networks to detect overconfidence effects and clinical tribalism and to assess learning motivation. Instruments included self-assessments for five learning dimensions (factual knowledge, skills, attitude, problem-solving and behaviour) and a four-item situational motivation scale. The analysis comprised paired t-tests, correlation analyses and two-step cluster analyses.
Results We detected overplacement, overestimation and signs of clinical tribalism. Responders in the physician subgroup rated themselves superior to colleagues and that their professional group was superior to other professions. Participants being educators in other competencies showed high overconfidence in health economics. We detected two groups of learners: overconfident but motivated persons and overconfident and unmotivated learners. Learning motivation did not correlate with overconfidence effects.
Discussion We could show the presence of overconfidence in health economics, which is consistent with studies in healthcare and the economy. The subjective perception of some medical educators, being role models to students and having a superior ‘attitude’ (eg, morality) concerning the economy may foster prejudice against economists as students might believe them. It also may aggravate moral distress and disrupts interactions between healthcare providers managers and leaders. Considering the study’s limitations, lifelong interprofessional and reflective training and train-the-trainer programmes may be mandatory to address the effects.
- behavior
- health education
- health economics
- quality in health care
- rationing
- risk management
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
National and multicentre sampling.
Numerically small sample size in a convenience sample setting.
Adequate power results due to partially high effect sizes.
Introduction
Background and rationale
Lifelong learning is a core competency of all healthcare providers.1 Learning applies to core competencies of a particular specialty (eg, surgery, dermatology or emergency medicine) and skills and knowledge in auxiliary but multiprofessional and multidisciplinary areas. These are, for instance, patient safety, workplace safety and data safety. Health economics is a supplementary but dominating field in daily practice for most healthcare providers. It focuses on hospital administration, distribution of limited financial and personal resources, hospital planning and development, financial risk management, and hospital leadership. Typically, economists in hospitals are directors and managers guiding healthcare professionals and making strategical decisions. This typically affects the dependent and (subjectively) ‘powerless’ healthcare workers.
Learning motivation in health economics is crucial to attending training formats and gathering and maintaining expertise for efficient communication and collaboration, ensuring patient, workplace and institutional safety. For healthcare providers in leadership positions, incompetence, malpractice and medical error in health economics may endanger all three safety areas,2 for example, when financial support is erroneously allocated away from efficient or critical to inefficient projects.
In times of staff shortage, ageing, technological complexity and ecological and geopolitical threats to the healthcare systems, unsafe care due to medical error is an additional risk, accounting for about 15% of medical investments.3 Consequently, learning is mandatory to raise patient safety and lower risk for healthcare systems. Unfortunately, subjective self-assessment of learning needs is a poor predictor of objective competence4–6 and is prone to bias-like overconfidence effects.
Overconfidence effects consist of different entities: overplacement (the belief to be better than others), overestimation (the belief to be better than tests reveal) and overprecision (the belief to know the truth).6 An additional effect is the in-group bias of the clinical tribalism phenomenon (the belief that the own group is superior to other groups).7 In healthcare, our working group detected these effects in different settings concerning hand hygiene,8–11 basic life support,12 second victim management,13 dysphagiology (under review), and point of care ultrasound (under review). Four of these studies revealed three different types of motivated learners: motivated, confident and competent ‘experts’, motivated but overconfident ‘recruitables’, and amotivated as well as overconfident ‘unawares’.12 13
In economics and finances, there are various studies on overconfidence, for example, in Chief Executive Officers (CEOs)14 15 and corporate and bank failure.16 17 To our knowledge, there is no evaluation of overconfidence in the discipline of health economics yet, and there are no studies about overconfidence and its contribution to learning motivation in medical economics either.
Thus, we postulated that it is also detectable in health economics.
Furthermore, while one might expect that overconfidence would lead to low learning motivation (‘I am the best! Why should I attend training?’), our preceding studies on the three clusters of learners in other medical competencies showed that this was not true, with some confident experts staying motivated and poor providers losing all motivation to learn. This phenomenon is known as the Matthew effect.18 19 In sum, the different overconfidence effects in health economics and their link to learning motivation remain unknown. This knowledge gap is even more prominent as learning motivation and competence are not simple entities:
According to the self-determination theory, motivation can be subdivided into intrinsic motivation (I want to learn), identified regulation (I have to learn, as I am a specialist), extrinsic motivation (my boss urges me to learn) and amotivation (I do not want to learn).20 One method of measuring motivation, according to Deci’s theory, is the Situational Motivation Scale (SIMS), which was initially validated for physical education.21 According to the revised Bloom’s taxonomy, learning to gain competence can be divided into the dimensions of ‘factual knowledge’ (eg, knowing about different tax laws), ‘psychomotor skills’ (eg, calculating cashflow from numbers), ‘attitude’ (eg, aspects of morality and ethics on economics), ‘problem-solving’ (eg, what can I do, when laws of two countries differ?) and ‘behaviour’ (behaviour on economy in real life).22 23
To gather more information about the interaction of learning motivation and overconfidence and whether we face a prototypical learning phenomenon in medical education, we transferred our methodology from previous fields (hygiene, life support, second victim phenomena, dysphagiology and sonography) to health economics.
Objectives
In this project, we focus on the occurrence and interaction of overconfidence effects and learning motivation in health economics. We hypothesised:
Overplacement effects are detectable in the learning dimensions of factual knowledge, psychomotor skills, attitude, problem-solving and behaviour concerning health economics. Overplacement is suggested when subjective assessments of one’s own and assessment of others differs in favour to self-assessment.
Overestimation effects are detectable in factual knowledge in health economics, suggested when self-assessment is above average, but a knowledge test on economic basics differs from the results of a group of experts.
Clinical tribalism effects are detectable in health economics for the five learning dimensions. Clinical tribalism is suggested when assessment of the own professional group and the assessment of other professionals differs in favour to the own profession.
Learning motivation in health economics can be detected in three patterns (experts, recruitables and unawares) as in previous studies.
Methods
We conducted a cross-sectional convenience sampling online survey among healthcare providers in Germany. We developed the survey with 27 questions in a group of three physicians (MB, SBu, SBe), one psychologist (MTK) and one physician who graduated in economy and quality management (RS) to ensure face and content validity. Internal consistency was assessed post hoc. The study population included healthcare providers from all professions, at least three regions (Hamburg, Munich, and Constance), and included undergraduates and postgraduates. We recruited additional participants via personal networks and social media boards with or without links to health economics (Xing, LinkedIn, Facebook). All data available were used. IP addresses were blinded towards the investigators. The data were regularly screened for survey fraud and other biases.24
Variables included demographic and psychometric data, self-assessment in health economics concerning five taxonomic learning dimensions, assessment of other medical staff concerning five taxonomic learning dimensions, measurement of learning motivation, estimation of risks according to ISO 3100025 and adapted k-prim questions on medical economics to assess factual knowledge: These questions comprise statements with questions whether they are either true or false or not known26). A version using the AI translation engine DeepL of the German questionnaire is available in online supplemental file A. Core questions about the assessment of own competencies of those of others are shown in box 1.
Supplemental material
Translation of the 20 core questions of the study assessed the 5 learning dimensions. Participants answered the five questions about their competencies and five each about the competencies of other persons: physicians, nurses and managers. Answers were given on a 7-point Likert scale.
Please answer the questions related to your competencies in the application of medical economic skills and methods (eg, preparing and evaluating balance sheets and performance measures, preparing and handling billing statements, controlling skills, personnel discussions, quality and risk management, marketing strategies, hospital and practice management, logistics, healthcare organisation, insurance systems).*
I have technical knowledge of these methods.
I am well-trained in the practice of these methods.
My attitude towards these methods takes patient safety into account.
When I use these methods, I can improvise.
I use these methods all day long.
Please answer the questions related to the competencies of medical professionals in the application of medical economic skills and methods
They have technical knowledge of these methods.
They are well trained in the practice of these methods.
Their attitude towards these methods takes into account patient safety.
When they use these methods, they can improvise.
They use these methods all day long.
Please answer the questions related to the competencies of nursing professionals in the application of medical economic skills and methods
They have technical knowledge of these methods.
They are well-trained in the practice of these methods.
Their attitude towards these methods takes into account patient safety.
When they use these methods, they can improvise.
They use these methods all day long.
Please answer the questions related to competencies MANAGEMENT PERSONNEL in the application of medical economic skills and methods (eg, preparation and evaluation of balance sheets and performance measures, preparation and handling of accounts, controlling skills, personnel discussions, quality and risk management, marketing strategies, hospital and practice management, logistics, healthcare organisation, insurance systems).*
They have technical knowledge of these methods.
They are well trained in the practice of these methods.
Their attitude towards these methods takes into account patient safety.
When they use these methods, they can improvise.
They use these methods all day long.
Questions marked with an asterisk (*) were mandatory questions.
We used an ascending seven-point Likert scale to assess the learning dimensions for oneself and others and the four items on learning motivation. The risk assessment included an ascending ordinal scale (minor, small, severe, critical and catastrophic effect).
Measurement
The survey included seven demographic items about sex, age, profession, educational grade, education in economics and current workplace. Question 8 was the Big Five Inventory-10,27 measuring the five psychometric properties using a 5-point Likert scale. Question 9 was a short version of the SIMS scale21 measuring the four dimensions of motivation by single items. Questions 10–13 comprised five items using a 7-point Likert scale each assessing the taxonomic learning dimensions (knowledge, skills, attitudes, problem-solving and behaviour) for the self and assessment of other physicians, nurses and hospital managers. Other professional groups were not assessed due to the response burden. Questions 14–17 comprised questions about the maximum credible harm for patient safety, hospital safety and witnessed occurrence.28 Questions 18–27 were modified k-prim questions (true/false/do not know) about different aspects of health economics created by the leading investigator according to the German Master of Health Economics curriculum and checked by two external medical economists. We counted false answers and ‘do not know’ as incorrect answers. Persons interrupting the questionnaire at this point were assigned zero points as would be done in educational testing. We excluded participants quitting the questionnaire at an earlier stage of progress before the overestimation analysis.
Statistics
Statistics included data processing and evaluation using Microsoft Excel (Microsoft, Redmond, Washington, USA) and SPSS V.28.0 (IBM).
We calculated the internal consistency of the questionnaire using Guttman’s criteria and Cronbach’s alpha. We considered internal consistency to be adequate for r>0.6. Additionally, we assessed the quality and consistency of the k-prim questions using discriminative power by Spearman correlations. We assumed good question quality for ρ>0.3.29
We tested hypotheses 1–3 for physicians and nurses using paired t-test and effect size estimations (hedge-corrected Cohen’s D) with interpretation to Cohen.30 We also applied Bonferroni adjustments to the p values. We identified overplacement (hypothesis 1) when assessing answers for oneself compared with answers concerning persons of the same profession. Overplacement was assumed when persons rated themselves to be significantly better than others. We repeated this process for each of the five learning dimensions in health economics. Overestimation (hypothesis 2) was assumed for those persons without economical education estimating themselves to be well educated concerning factual knowledge, but scoring significantly lower in the knowledge test than those participants with economical education. Clinical tribalism (hypothesis 3) was assessed according to hypothesis 1 but by comparing the own occupational group with others. We conducted paired t-tests in this comparison for each of the learning dimensions, applying Bonferroni adjustments to the p values. We examined participant heterogeneity and aimed to group them into homogeneous clusters based on their knowledge assessment, motivation to learn, and performance on the knowledge test. This was accomplished through a two-step cluster analysis, treating the four motivational dimensions and the knowledge test as continuous variables. All continuous variables underwent automatic z-standardisation in the programme before analysis. The determination of the cluster count was not predefined; instead, the algorithm autonomously identified the optimal cluster solution (a maximum of 15 clusters was applied). The distance measurement employed was Euclidean distance. The analysis was repeated with different fit indices—Bayes information criterion and Akaike information criterion. Subsequently, we assessed the efficiency of the proposed cluster solution by reviewing the mean Silhouette coefficient for cohesion and separation. A Silhouette coefficient above 0.25 is deemed sufficient, and values exceeding 0.45 are considered good. The correlations between overconfidence and the analysis of the influence of psychometric parameters were conducted using Pearson’s correlation analyses. To improve the robustness of estimations, SEs and CIs, we conducted bias-corrected bootstrapping with a CI of 95% based on 1000 samples.
Patient and public involvement
None.
Results
Questionnaire
We assessed the quality of the questionnaire post hoc. The reliability was sufficient with Guttman’s criteria (λ−1 to λ−6) ranging from 0.83 to 0.96 and a Cronbach’s alpha of 0.94. K-prim questions showed good discriminative power for economic key figures (ρ=0.7, p<0.001), the political composition of the German Federal Joint Committee (G-BA) (ρ=0.87, p<0.001), hospital finances (ρ=0.66, p<0.001), quality indicators (ρ=0.72, p<0.001), diagnosis-related group calculation (ρ=0.8, p<0.001), legal regulation of working time (ρ=0.49, p<0.001), stakeholder analysis (ρ=0.76, p<0.001), shareholder analysis (ρ=0.7, p<0.001), billing regulations (ρ=0.78, p<0.001) and medical patent protection (ρ=0.78, p<0.001).
Participants
Altogether 116 participants (32% male, 0% non-binaries or others each) responded, with 66 completing the whole questionnaire. Age ranged from 22 to 68 years (mean 42.5 years, SD 10.4). Of all participants, 49 were nurses (42.7%), 38 (32.8%) physicians, 22 paramedics (19%) and 7 other medical professionals. 20 persons (17.2%) were educated in medical economics previously, and 9 were still training in economics during the survey.
Results on overplacement
Physicians (n=29) assessed themselves (M=3.6, SD=1.9) to be better than others (M=3.1, SD=1.6) in factual knowledge about health economics (p=0.04, D=0.33). This was also the case in psychomotor skills in health economics (M=3.2, SD=1.7 for self and M=2.8, SD=1.6 for others) but with no significance (p=0.051, D=0.31), for the learning dimensions attitude (self: M=4.6, SD=1.8 others: M=4.0, SD=1.7) with medium effect size (p=0.015, D=0.42), problem-solving (self: M=3.5, SD=1.6, others: M=3.3, SD=1.7) missing significance (p>0.05, D=0.21) and behaviour (self: M=2.7, SD=1.6. others: M=2.2, SD=1.2) with medium effect size (p=0.025, D=0.37). The results for the three main professions (physicians, nurses, economists) rated by physicians are available in figure 1.

Assessment of competencies by physicians compared with other physicians. The x-axis shows the five learning dimensions with bars for self-assessments (blue) and other physicians (orange). The y-axis shows mean estimations on the 7-point Likert scale (0–6). Asterisks (*) indicate significant results.
Physicians lacking economic education assessed themselves as inferior to those with completed education in health economics (p<0.001 for ‘factual knowledge’ with M=3.27 and SD=1.6 for self and M=5.14 and SD=1.6 for others. p<0.001 for ‘psychomotor skills’ with M=2.73 and SD1.6 for self and M=4.93 SD=1.9 for others, p=0.008 for ‘attitude’ with M=4.23 SD=1.8 for self and M=5.8 SD=1.0 for others and p=0.003 for ‘behaviour’ with M=2.6 SD=1.4 for self and M=4.0 SD1.6 for others), except for the dimension of ‘problem-solving’. In contrast, the physicians in training significantly rated themselves superior to inexperienced physicians and postgraduates in health economy (p=0.018). Results are shown in table 1.
Assessments of 29 physicians and comparison of their estimation for their own competencies compared with others.
In 26 nurses, we could not detect differences in assessing their and other nurses’ competencies in all 5 learning dimensions (p>0.05). Our questionnaire only assessed the competencies of physicians and nurses, not other healthcare providers. In summary, hypothesis 1 (testing the presence of overplacement) was confirmed for physicians but not for nurses.
Results on overestimation
Overestimation (that could only be measured for knowledge in this study) could be confirmed for 23 persons of all professions without formal economic education but mostly or strongly agreeing with the item on being well educated in economics. This group strongly agreed to have good factual knowledge and scored significantly (p=0.045) fewer points in the factual knowledge test (M=12.18, SD=15.2) compared with educated responders with high self-assessment (M=27.3, SD=11.9). Consequently, hypothesis 2 testing overestimation could be confirmed.
Results on clinical tribalism
The results on clinical tribalism are available in figures 2 and 3. Physicians rated their occupational group to be better educated in economics in all learning dimensions than nurses with high effect sizes for factual knowledge (M=3.11, SD=1.7 vs M=2.2, SD=1.1, p=0.002 and D=0.7), psychomotor skills (M=2.8 SD=1.5 vs M=1.9, SD=1.1, p=0.003 and D=0.79), attitude (M=3.9, SD=1.7 vs M=2.6, SD=1.2, p=0.003 and D=0.8) and problem-solving (M=2.2, SD=1.1 vs M=1.8, SD=1, p=0.011 and D=0.6).

Physicians rating their own (Phys-Phys) nurses’ (Phys-Nurse) and economists' (Phys-Oec) aspects of competence. The x-axis shows the five learning dimensions with bars for physicians rating physicians (blue), nurses (orange) and economists (grey). The y-axis shows the mean estimations on the 7-point Likert scale.

Nurses rating their own (Nurse-Nurse), physicians (Nurse-Phys) and economists’ (Nurse-Oec) aspects of competence. The x-axis shows the five learning dimensions with bars for physicians (blue), nurses (orange) and economists (grey). The y-axis shows mean estimations on the 7-point Likert scale.
Compared with economists, physicians rated their colleagues to be inferior in knowledge (M=3.11; SD=1.7 vs M=4.3; SD=1.8, p=0.002, D=0.61), skills (M=2.8, SD=1.5 vs M=4.0; SD=1.7, p=0.001, D=0.6) and behaviour (M=2.2, SD=1.1 vs M=4.1; SD=1.8, p<0.001, D=1.0). For problem-solving, there was no significant difference (M=3.25, SD=1.7 vs M=3.7; SD=1.5; p>0.05, D=0.06), for attitude physicians rated themselves to be superior to economists (M=3.9, SD=1.7 vs M=2.9; SD=1.5, p<0.002, D=0.6).
Nurses estimated their occupational group slightly superior to physicians in knowledge (M=4.15, SD=1.4 vs M=3.7; SD=1.6, p>0.05, D=0.4), skills (M=3.7, SD=1.6 vs M=3.4; SD=1.6, p>0.05, D=0.3) and behaviour (M=3.35, SD=1.4 vs M=2.9; SD=1.5, p=0.051, D=0.33) partially with near misses in significance. For problem-solving (M=3.7, SD=1.6 vs M=3.2; SD=1.8, p=0.036, D=0.36) and attitude (M=4.81, SD=1.7 vs M=4.1; SD=2.0, p=0.006, D=0.52) nurses rated themselves superior to physicians.
Compared with economists, nurses rated their factual knowledge (M=4.15, SD=1.4 vs M=4.5; SD=1.7, p>0.05, D=0.16) and skills (M=3.7, SD=1.6 vs M=4.2; SD=1.9, p>0.05, D=0.19) to be inferior compared with economists, missing significance but with small effect sizes towards economists’ superiority. They rated themselves superior in problem-solving but missing significance (M=3.8, SD=1.7 vs M=3.6; SD=1.8, p>0.05, D=0.13). For attitude, they rated themselves to be inferior (M=3.35, SD=1.4 vs M=3.9; SD=2.0, p>0.05, D=0.25). As in physicians, nurses rated themselves as superior in attitude compared with economists (M=4.81, SD=1.7 vs M=4.1; SD=1.9, p=0.016, D=0.44).
Consequently, and especially regarding the learning dimension ‘attitude’, overplacement of the own occupational group above other groups and an expert group was confirmed, thereby validating hypothesis 3, that is, the presence of clinical tribalism.
Cluster analysis
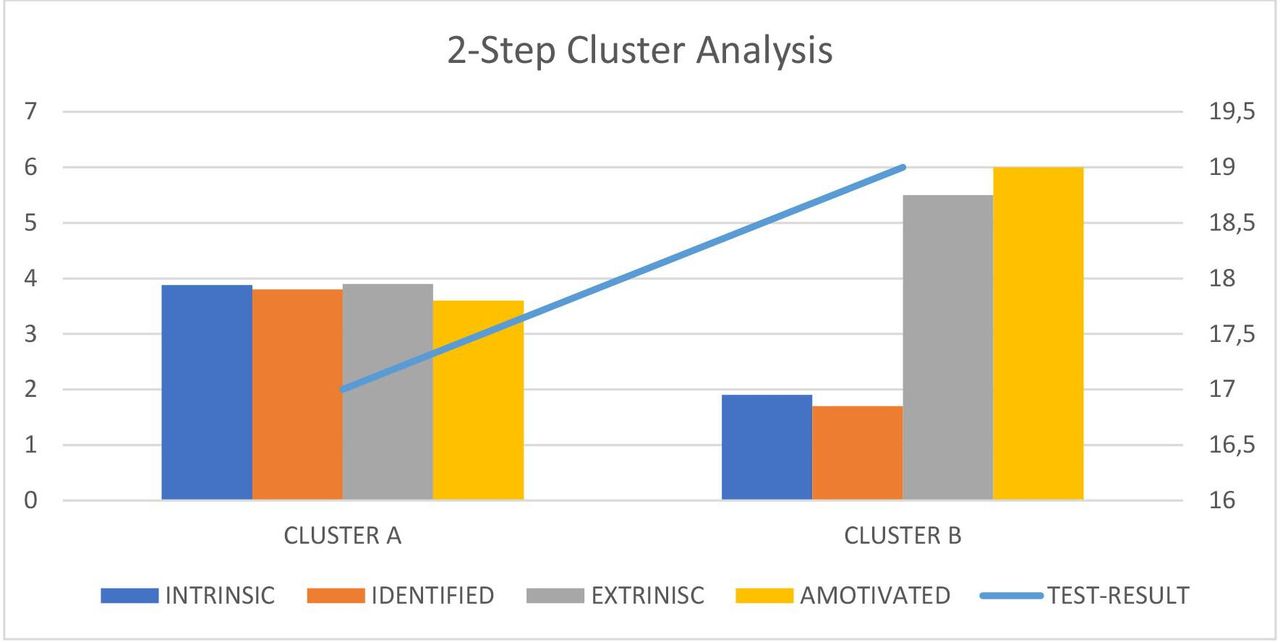
We identified two clusters using the two-step cluster analysis, with an appropriate Silhouette coefficient(see figure 4): cluster A showed average intrinsic motivation (M=3.88; SD=1.2), identified regulation (M=3.9, SD=1.9), extrinsic motivation (M=3.9, SD=1.9) and amotivation (M=3.6; SD=1.67). Participants showed a mean test result of 17 (M=17.2; SD=12.3). Cluster B was not intrinsically motivated (M=1.9; SD=0.7), not identified regulated (M=1.7; SD=0.8), strongly extrinsically motivated (M=5.5; SD=1.4) and amotivated (M=6.0, SD=1.1) with a slightly higher test result (M=19.0; SD=13). No demographic differences except for age and extraversion were found between the clusters: persons in cluster B were older than in cluster A (M=45.4; SD=9.9 vs M=40, SD=10.1, p=0.036) and had higher extroversion (p=0.033). Participants in cluster B rated risk to institutions in case of an economic error higher than in cluster A (low risk 0 vs 1, moderate risk 16 vs 6, critical 6 vs 27 and catastrophic 2 vs 8 participants in clusters A and B). This was reproducible for potential harm to patients (low risk 2 vs 0, moderate risk 8 vs 13, critical 13 vs 22 and catastrophic 1 vs 7 participants in cluster A and B). Nobody rated the risk to be ‘minor’.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cluster formation. The left y-axis showed motivation results (7-point Likert with 7=maximum motivation and 1=no motivation), and the right y-axis shows test results in points (blue graph). X-axis shows cluster A (‘recruitables’) and B (‘unawares’) with different motivation dimensions: intrinsic (blue), identified regulated (orange), extrinsic (grey) and amotivated (yellow).
Consequently, our hypothesis assuming three clusters was rejected.
Additional tests
In addition to the main results, we tested correlations between self-assessment, learning motivation and psychometric characteristics but could not detect significant strong correlations (p<0.05 and r>0.6) using a Pearson correlation. We detected a weak positive correlation between the level of self-assessment in knowledge and extraversion (r=0.28, p=0.007) and a negative correlation to intrinsic motivation (r=0.27, p=0.01) and identified regulation (r=0.26, p=0.013). Concerning skills, we detected weak and moderate correlations to extraversion (r=0.028, p=0.007) and openness (r=0.3, p=0.004) and a negative one towards intrinsic motivation (r=0.23, p=0.028). This was reproducible for attitude correlating weakly with extraversion (r=−0.26, p=0.013), openness (r=0.21, p=0.045), intrinsic motivation (r=0.38, p<0.001) and identified regulation (r=0.36, p<0.001). For problem-solving, we could detect this only for extraversion (r=0.28, p=0.006). Regarding behaviour, we found a weak correlation to openness (r=0.29, p=0.005) and intrinsic motivation (r=0.2, p=0.006). Openness was correlated positively with age (r=0.3, p=0.004).
The risk assessments showed that 1% of the participants rated the maximum credible harm to a health institution in case of an economic decision error of minor effect. Other participants rated this to be moderate (34%), critical (50%) or catastrophic (15%). Regarding patients, respondents rated errors in the economy to be of minor effect (2%), moderate effect (32%), critical effect (54%) or lethal (12%).
Of the 116 participants, 27 stated that they were educators in some field of healthcare. Of these, 9 rated themselves as well educated in ‘factual knowledge’ and 18 in ‘attitude’, with 5 giving themselves the highest rating. All five persons showed test results under 10 points—lower than the mean of all other participants.
Discussion
Key results
This is the first study on overconfidence effects in health economy and learning motivation. We detected overplacement effects in physicians, overestimation in physicians and nurses, and clinical tribalism in physicians and nurses, especially concerning the learning dimension attitude—partially confirming hypotheses 1, 2 and 3. However, we detected two learning patterns, instead of the three predicted—rejecting hypothesis 4. Further, we could not detect a robust correlation between learning motivation and overconfidence.
The responders’ risk estimations correctly show how errors in the health economy may impact institutions and even individuals, with most of the respondents rating economic errors as catastrophic for hospitals (eg, insolvency) and patients (eg, lifelong impairment or death). These individual and subjective ratings of risks are in concordance with institutional risk assessments on economics (that are based on actual numbers and may be more objective). Consequently, preserving the motivation to learn to maintain competencies in health economics is essential for healthcare providers (especially in leadership positions) to ensure patient and institutional safety.
The results on overplacement, overestimation and clinical tribalism are concordant with findings in medicine and economy: in medicine, several working groups detected overplacement and overconfidence in different medical areas and proficiencies.8–13 31 32 Similar findings could be demonstrated in the economy, politics and education.4 5 14 16 17 33–38 Therefore, our findings show validity towards the robustness of the effect on the health economy. A new aspect of our study is that overconfidence (especially overplacement) varied in the five learning dimensions described by Bloom. Consequently, future studies should differentiate between assessments of their own and others’ competencies in several dimensions rather than as a whole competency.
Further, we detected that nurses and physicians judged their own ‘attitudes’ (which focus on inner values, morality and ethics, eg, how resources are distributed) concerning the health economy more than economists. This might lead to the disruptive dilemma that medical staff (with presumably high experience in healthcare and low competence in economics) postulate that economists (with presumably little experience in patient contact but high competence in economics) cannot use their competencies ethically. This feeds the narrative of ‘bad and greedy economists and hospital managers’ and may provoke moral distress,39 moral injury40 or burn-out,41 moving healthcare providers out of hospitals. Aggravation of staff shortage follows and provokes rationalisation and even triage. However, this study could not test for overestimation in attitude as we only tested this for ‘factual knowledge’.
Concerning educators in other medical fields that have poor competencies in economics, it might be possible that these are overconfident medical educators: They usually teach a different specialty but may teach aspects of health economics wrongly and thus influence students with a halo effect (‘(S)he is a good teacher about XY, so (s)he must know something about economics too’).42
In previous studies, we detected three different learning patterns: confident and motivated learners (experts), overconfident motivated learners (recruitables) and overconfident unmotivated learners (unawares). In this study, we detected two clusters (A and B) that are attributable to ‘unawares’ (B) and ‘recruitables’ (A). The ‘expert’ group is missing. This may be due to the small sample size, reduction of the SIMS instrument or motivational factors to participate in the survey. This finding differs from most of our previous studies, except one study on dysphagia management, which also detected only two patterns (‘experts’ and ‘recruitables’ but not ‘unawares’), and one study on second victims13 that only showed slight differences between the clusters.
In contrast, we could detect a strong differentiation between these clusters in life support12 and hand hygiene.11 On the one hand, this might be a problem of sample size or, on the other hand, a problem of proficiency that is very distinct for life support and hand hygiene. In contrast, second victim, dysphagiology and economics are broader ‘fields’ of expertise. Consequently, future work should clarify these effects and the role of overconfidence in expertise fields and distinct tasks.
Future work should concentrate on the question of how to manage the involuntary effects of overconfidence and clinical tribalism, which need to be distinguished from intended arrogance. Interprofessional education is known to lower clinical tribalism43 and reflective learning lowers overconfidence by triggering metacognition.44 Both require effective and efficient train-the-trainer programmes using reflective and interprofessional concepts rather than passive lessons and or readings.45 Additionally, programmes for educators should teach how to maintain resilience, patience and grit46 to resist the frustration of unwilling or absent learners.
Limitations
Our study faces several limitations. First, because of the small sample size47 and convenience sampling24 from social media, the results cannot be generalised to the whole population provided with the survey. Hence, to increase generalisability, the study should be replicated in closed populations. However, it is important to note that our primary intention was to identify effects rather than collect epidemiological data. Consequently, the small sample size limited our ability to detect small and medium effects in the current study. To detect small and medium effect sizes, confirming studies should be conducted in more extensive samples with a minimum response rate of 60%.48
Second, we used factual knowledge for overestimation testing. Testing overestimation for skills would have required other formats, for example, objective structured clinical examinations (OSCE) testing skills or situational judgement tests evaluating ‘attitude’ (personal values, morality and ethical context), leaving room for future studies. In our scoping study, we did not implement these for the concern of response burden.
Third, we measured learning motivation using a reduced version of the SIMS of only 4 instead of 16 items. This might be beneficial and even raise validity,49 but critical findings on learning motivation should be treated with caution.
Fifth, we counted the answers with zero points if they were answered falsely or left out. De facto, we do not know why people quit the test (no motivation to be tested, offended at being tested, unwanted reflection, no time, etc), but counting zero points for an interrupted or unfinished test is a common procedure in education and testing.
Sixth, we identified overestimation effects when comparing participants with all healthcare professionals for factual knowledge, but not within the subgroup of physicians that showed lower estimates in persons without economic education than those with education. These contradictory findings might be biased by a sample size error or by different in-group and out-of-group effects assessing overconfidence and by the findings that persons tend to overestimate themselves in tasks on the one side and overplacing them simultaneously on the other.6 Consequently, large-scale studies should focus on this point as it seems to be relevant to the methodology of overconfidence assessments.
Seventh, we only analysed the effects for nurses and physicians, but not for paramedics and other professionals leaving space for further investigations. We decided to do so as a cross-sectional assessment of all professions for clinical tribalism would have lengthened the questionnaire and would have increased the response burden.
Interpretation
We conclude that we detected overplacement in health economics, closing the gap between overconfidence in economics and healthcare. Moreover, this is the first study revealing differences in overconfidence in the five learning dimensions. Consequently, future educational tests on overconfidence should address these dimensions separately. This does not only apply to overplacement, but to overestimation as well, with the need for different test formats, for example, knowledge testing for factual knowledge, OSCE skill testing, situational judgement tests for attitude and direct observation of practical skills evaluating problem-solving and behaviour. However, it remains unclear whether and how the differences between overplacement and overestimation interact with learning motivation and lifelong learning and how they could be addressed by curriculum developers, educators and trainers.
Additionally, the role of ‘unaware’ teachers who overestimate their competencies in a particular field like economics must be examined and risk stratified as they may unintentionally teach false content under a halo effect. This and the aspects of medical professionals rating themselves higher in attitude compared with economists might lead to distress, disruptive group effects in hospitals, further economic or medical error, science myths and legends, and (if ever identified) the resourceful demand for corrective training and train-the-trainer programmes. In times of low resources and recent challenges to healthcare and economics, medical education researchers should concentrate on these questions to enforce efficiency, quality and learning safety as a foundation for patient, workplace and institutional safety in trainees and experts.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but ethics committee of the physicians association of Baden-Wurttemberg, Stuttgart, Germany exempted this study. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The authors contributed to the study as follows: SBu: conceptualisation, recruitment, statistics, primary draft of the manuscript, guarantor. MB: conceptualisation, pretesting, recruitment, primary draft of the manuscript. SBe: pretesting, recruitment, primary draft of the manuscript. OS: supervision, validation. RS: conceptualisation, supervision, validation, primary draft of the manuscript. HM: recruitment, primary draft of the manuscript. FH: recruitment, primary draft of the manuscript. MT-K: statistics, supervision, primary draft of the manuscript. BG: validation, primary draft of the manuscript, native speaker (English). All authors approved the final version of the manuscript. We used 'Grammarly' for writing the first draft. This is an AI-assisted software assisting in orthography, interpretation and assisting in grammar questions and corrections. The programme was not used to generate texts or passages and not in reference search, methodology, analysis or interpretation of our work. Otherwise, we did not use AI technology.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.