Article Text

Abstract
Objectives Identifying whether a country is ready to deploy a new vaccine or improve uptake of an existing vaccine requires knowledge of a diverse range of interdependent, context-specific factors. This scoping review aims to identify common themes that emerge across articles, which include tools or guidance that can be used to establish whether a country is ready to deploy a new vaccine or increase uptake of an underutilised vaccine.
Design Scoping review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews guidelines.
Data sources Embase, CINAHL, Cochrane Library, Google Scholar, MEDLINE, PsycINFO and Web of Science were searched for articles published until 9 September 2023. Relevant articles were also identified through expert opinion.
Eligibility criteria Articles published in any year or language that included tools or guidance to identify factors that influence a country’s readiness to deploy a new or underutilised vaccine.
Data extraction and synthesis Two independent reviewers screened records and performed data extraction. Findings were synthesised by conducting a thematic analysis.
Results 38 articles met our inclusion criteria; these documents were created using methodologies including expert review panels and Delphi surveys and varied in terms of content and context-of-use. 12 common themes were identified relevant to a country’s readiness to deploy a new or underutilised vaccine. These themes were as follows: (1) legal, political and professional consensus; (2) sociocultural factors and communication; (3) policy, guidelines and regulations; (4) financing; (5) vaccine characteristics and supply logistics; (6) programme planning; (7) programme monitoring and evaluation; (8) sustainable and integrated healthcare provision; (9) safety surveillance and reporting; (10) disease burden and characteristics; (11) vaccination equity and (12) human resources and training of professionals.
Conclusions This information has the potential to form the basis of a globally applicable evidence-based vaccine readiness assessment tool that can inform policy and immunisation programme decision-makers.
- Public health
- INFECTIOUS DISEASES
- Health Equity
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. The completed data extraction form, which is the source data for results figures and tables, is publicly available on GitHub, along with the code required to generate the results: https://github.com/lukebax/readiness.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The scoping review used a comprehensive search for articles in peer-reviewed journals, with all search strategies being independently peer-reviewed using the PRESS checklist.
Synthesising data from national and international vaccine readiness tools and various guidance documents provided a methodology to create an evidence-based framework with broad applicability that can be used to assess a country’s vaccine readiness.
Similar concepts were described in a myriad of ways making data synthesis a challenging and iterative process.
The comprehensive search strategy (that considered over 6000 articles across 7 databases) was unable to find 10 specific documents that had been preidentified as relevant, therefore, some articles were manually identified through expert input.
Introduction
The development of new or improved vaccines is a key vehicle to improve health outcomes across the world, with follow-on benefits to equity, economic capacity and societal function.1 2 With the emergence of new diseases (eg, COVID-19),3 or the resurgence of existing diseases (eg, polio),4 the importance of rapid introduction or reintroduction of vaccines is increasingly evident. Effective roll-out of vaccines is critical to their success—particularly where high levels of vaccination are required to control transmission.5
Vaccine roll-out is affected by a multitude of interacting factors at local, district, country and regional levels. These factors are driven by both the supply (eg, distribution) and demand side (eg, individual willingness to receive a vaccine). They incorporate logistical factors, governmental healthcare systems, policy and social perceptions including confidence in vaccination, which may have been influenced by misinformation and disinformation. The combination of these factors creates an overall assessment of ‘vaccine readiness’ for a particular region or group. For example, in the last 10 years, 86 countries have introduced rotavirus vaccines (increasing from 30 countries in 2011 to 116 countries in 2021).6 After the introduction, global coverage of the rotavirus vaccine increased from 9% in 2011 to 51% in 2022.7 However, these statistics are underpinned by significant variability between countries.8 For example, as of January 2022, rotavirus vaccines have been introduced in national immunisation programmes in 79% of sub-Saharan African countries, 60% of countries in the Americas and in only 46% of countries in southeast Asia.9 This variability is underpinned by a multifaceted set of interdependent factors.
The ability to assess a country’s vaccine readiness for a particular vaccine is valuable for several reasons: it allows countries to self-assess and prioritise areas for improvement; it allows overarching bodies (eg, the WHO or European Commission) to identify deficiencies (or weaknesses) to prioritise support; it allows external organisations, such as non-governmental organisations to focus their efforts for greatest impact. More importantly, many factors affecting vaccine readiness are amenable to country-level intervention, including through communications and public information strategies.
Recent work led by international organisations, and influenced by the impact of the COVID-19 pandemic, has aimed to define the factors that influence country-level vaccine readiness. Work conducted by COVAX, co-led by the Coalition for Epidemic Preparedness Innovations, the Vaccine Alliance, Gavi and the WHO, alongside key delivery partner UNICEF, has shown that our ability to achieve vaccine coverage targets requires effective planning, coordination and implementation strategies.10 Multiple documents, including tools and decision-making platforms, have been created to aid evaluation during the COVID-19 pandemic.11 For example, WHO-UNICEF issued a COVID-19 National Deployment and Vaccination Plan12 to support countries to decide whether national readiness to deploy a specific vaccine has been established. However, readiness in a pandemic setting needs to consider specific factors, such as political prioritisation, time-scrutiny, emergency authorisations and regulatory process changes, rapid updates from governments, access to emergency funding and more. Consequently, the recent focus on deploying COVID-19 vaccines is not necessarily generalisable and leaves a gap when considering readiness for the deployment of new routine vaccines or improving uptake of underutilised vaccines in national vaccination schedules.
Therefore, there is a system-level evidence gap in the resources available to enable rigorous, comprehensive assessment of vaccine readiness (whether for new vaccines or to improve uptake of underutilised vaccines).13 A variety of guidance documents have been developed, of which many relate to the use of specific vaccines or specific target populations,14 while other documents consider the use of vaccines in a more general context.15 These guidance documents have been created using different methodologies, targeting various geographical regions and vaccine types. To date, there does not appear to be a globally applicable, comprehensive vaccine readiness assessment approach that can be applied widely, across all vaccine types, populations and geographies. We believe there is an urgent need for an evidence-based tool to fill this gap.
We, therefore, conducted a scoping review to identify existing guidance used to assess whether a country is ready to roll out a new vaccine or support enhanced uptake of an existing vaccine. This review had two aims. The first was to identify current tools, guidelines, checklists or other relevant documents that have been developed to support decision-making in relation to whether a country is ready to deploy a vaccine or improve uptake of an underutilised vaccine. The second aim was to establish common themes and subthemes that arise across these documents. This enabled us to identify a set of universal factors suitable to underpin the development of a comprehensive, broadly applicable, evidence-based tool to assess vaccine readiness. We propose that such a tool could be a foundational platform to support enhancements to vaccine roll-out for new and underutilised vaccines, and therefore, population health. Further, enhancements could have a synergistic effect on the overall performance of the immunisation programme and ecosystem more broadly.
Methods
Search strategy and selection criteria
Our review protocol was written according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocol (PRISMA) guidelines16 17 and was originally registered on the Open Science Framework18 on 14 April 2023 (https://doi.org/10.17605/OSF.IO/64Q8M). Subsequently, changes to the protocol were made to clarify the review aims and broaden the literature search. A revised protocol indicating all updates from the original version (with tracked changes) is available on OSF (https://doi.org/10.17605/OSF.IO/WGNFP).
We conducted the review using the Arksey and O’Malley framework19 and report information in line with PRISMA for Scoping Reviews guidelines.20 The research question that we addressed was what are the common themes across tools that can be used to assess a country’s readiness to deploy a new or underutilised vaccine? Our review question is presented in PICO (Population, Intervention, Comparison, and Outcome) format in online supplemental table S1.
Supplemental material
Our eligibility criteria are tabulated in online supplemental tables S2 and S3. We included studies and other documents that detailed country-level tools and guidance documents that related to vaccine deployment. All study designs were included from any publication year and in any language. No further limits were applied.
We searched MEDLINE, Embase, PsycINFO, CINAHL, Cochrane Library (CDSR and CENTRAL), Web of Science (SCI-EXPANDED and SSCI) and the top 200 hits from Google Scholar21 on 9 September 2023. Our search strategies were independently peer-reviewed using the PRESS (Peer Review of Electronic Search Strategies) checklist22 by Kat Steiner and Matthew Henry, Outreach Librarians at the Bodleian Health Care Libraries, University of Oxford. All search strategies are presented in full in online supplemental information S1.3.
The search results were deduplicated and screened using EPPI-Reviewer Web (ER-Web).23 Study selection was a two-stage process: screening on title and abstract followed by screening on full text. Screening was carried out in duplicate by two independent reviewers and disagreements settled by discussion between both reviewers. Relevant tools or guidance documents that related to a country’s readiness to deploy a new or underutilised vaccine were also identified through expert opinion.
Data analysis
Characterising article types and data sources
After determining each guidance document’s eligibility, the following data were extracted: title, authors; date of publication; geographical scope, type or types of vaccine considered, in-text descriptor of how the information was gathered (eg, expert review, literature review, policy brief) and in-text descriptor of the content type that was generated (eg, checklist, tool, guideline, framework). We reviewed a wide-range of documents (collectively referred to in this scoping review as ‘guidance documents’) that were curated using a range of methodologies. Using this approach to gather and triangulate information across different sources provided the flexibility to draw conclusions across a wide pool of information.
Thematic analysis
A thematic analysis was conducted to identify and analyse commonalities that emerged across guidance documents, and to interpret patterns that arose across key themes. As Vaismoradi et al described,24 conducting a thematic analysis using a descriptive approach allows data reduction to be conducted in a flexible and positive way. Data synthesis was conducted whereby a list of themes and subthemes were developed that accurately reflected key factors associated with a country’s readiness to deploy a new or underutilised vaccine. First, key factors relating to vaccine readiness were extracted from each text and tabulated to inductively interpret the empirical material, through an iterative and reflexive process.25 These were collated to form a comprehensive list of key factors and synthesised to explore patterns identified across guidance documents, which would contribute to overarching themes. Factors relating to each theme were then grouped, and themes were reviewed to ensure clarity and consistency in terms of terminology and meaning. Assessments of the grouping within each theme were developed and reviewed through regular discussion in team meetings. Where required, themes were refined and redistributed to produce a final set of distinct and individual themes. Factors within each theme were then categorised to develop subthemes, which represented the scope of the theme. This enabled distinct overarching themes to be produced, with a core list of subthemes within each theme.
Patient and public involvement
None.
Results
Article selection and article characteristics
We identified 38 articles12–15 26–48 48–59 that were eligible for this review: 28 from databases and 10 from other sources identified through expert opinion. The article selection process is displayed in figure 1. Specific characteristics for each included article are presented in online supplemental table S4, with summaries of the characteristics presented in figures 2–3 and table 1, box 1 and online supplemental table S5 .

The Preferred Reporting for Systematic reviews and Meta-analyses (PRISMA) diagram representing the systematic literature search.

Characteristics of articles included in the review. (A) Publication year; (B) Vaccine type; (C) In-text description of approach used to gather relevant information; (D) In-text description of type of guidance document.

{kind=link}
{kind=link}
{kind=link}
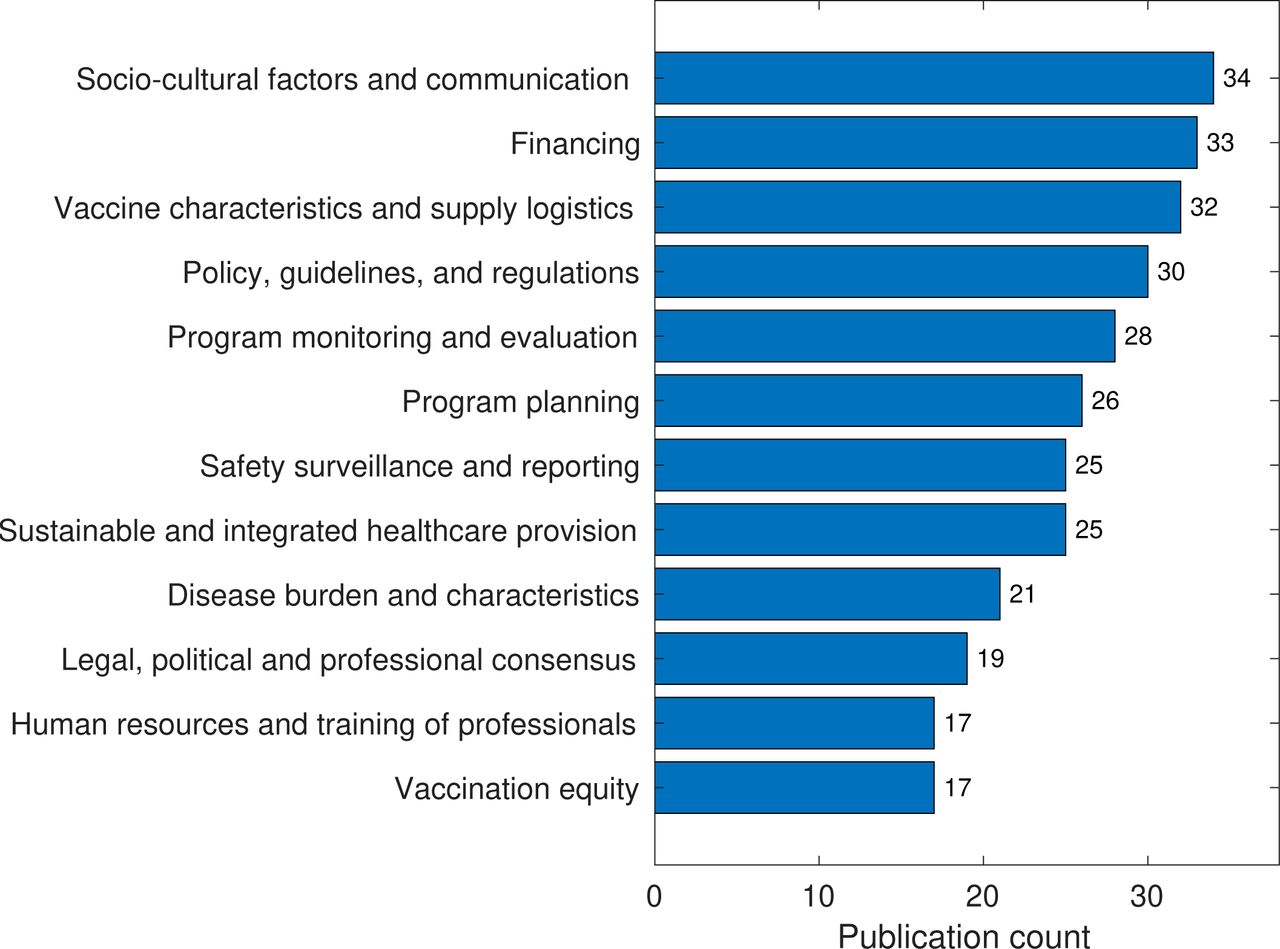
Summary of core themes, listed by number of included articles discussing each theme.
A summary description of each of the 12 themes
Subthemes of each theme that emerge across guidance documents
Legal, political and professional consensus
Establish a legal framework for vaccine deployment.
Determine political will for an immunisation programme.
Determine consensus for vaccine recommendation amongst medical and scientific communities.
Ensure commitment from stakeholders to support the immunisation programme introduction and continued deployment.
Create stakeholder advocacy and lobbying plans.
Confirm commitment to accurate and responsible data collection and sharing.
Sociocultural factors and communication
Consider the acceptability of the vaccines and any perceived risks.
Ensure development of a communication plan.
Ensure distribution of awareness campaigns, information dissemination (including media and social media) and public education.
Establish demand planning and demand generation strategies.
Consider social mobilisation strategies.
Policy, guidelines and regulations
Ensure conformity with established global guidelines.
Establish national guidelines and a consensus statement.
Ensure there is consensus between stakeholders.
Ensure the programme is standardised and verified.
Develop and enforce regulations and quality assurance processes.
Set up a regulatory mechanism to register and approve vaccines and ensure a quality system is in place.
Financing
Evaluate the cost-effectiveness of the programme (including government expenditure on vaccines and projected savings in healthcare) and ensure that this is within acceptable national thresholds.
Consider the cost to existing healthcare programmes.
Ensure there is adequate financing in place to initiate the immunisation programme, that is, to set up and introduce the programme.
Ensure there is adequate financing in place to maintain the immunisation programme.
Develop a strategy to ensure financial sustainability for the maintenance of the immunisation programme, that is, to ensure the long-term continuation of the programme.
Secure approval for immunisation programme costs in the government budget (eg, line items for the purchase of vaccines).
Vaccine characteristics and logistics
Consider vaccine pharmacological properties which may impact the design of an immunisation programme (eg, thermostability).
Conduct demand forecasting.
Set up storage and thermostability facilities.
Ensure an adequate transport system is available to deliver vaccines.
Organise a waste management system.
Consider overall logistics that is, designate a responsible party for ensuring that the physical vaccine is managed and administered appropriately, for example, overall coordination of storage and liaison with transport systems and vaccination centres, Personal Protective Equipment (PPE) management, security systems.
Coordinate supply of vaccine related consumables.
Arrange long-term supply of vaccines.
Programme planning
Create a national technical working group with terms of reference and roles and responsibilities.
Create a top-level organisation chart to establish roles and responsibilities within the programme.
Establish a scope, prioritisation and goal setting plan with a project timeline.
Prepare a vaccine introduction plan.
Create a macroprogramme and microprogramme plan and make decisions based on evidence.
Develop a long-term immunisation strategy, including catch-up and booster vaccines.
Programme monitoring and evaluation
Evaluate the short-term impact of vaccination on disease burden, and evaluate the long-term impact through epidemiological surveillance.
Ensure there is a management information system in place and have a mechanism to report data.
Develop a monitoring framework, or adapt an existing monitoring framework, to incorporate recommended advice and provide a mechanism to incorporate feedback.
Implement a monitoring plan to chart how the implementation and roll-out of the immunisation programme is progressing.
Supervise the implementation of the programme.
Establish a mechanism to evaluate the implementation of the programme, to ensure sustained immunity in the target population.
Use the programme to learn and improve understanding of deployment of a large-scale healthcare event, through developing Research and Development (R&D), conducting operational and/or effectiveness research and an impact assessment.
Sustainable and integrated healthcare provision
Country commitment to delivering a sustainable and effective immunisation programme (eg, demonstrable of good stewardship and implementation of national health plans, previous success of vaccine introduction).
Determine the relevance to the public health and public health value attributed to the programme.
Determine the likelihood of implementing the immunisation programme through a formal feasibility assessment.
Ensure a sustainable immunisation programme, which is resilient, fit-for-purpose and responsive.
Integrating the immunisation programme into existing healthcare programmes and current immunisation schedules.
Identify regional and geographical gaps in healthcare provision and develop a plan to create equal access to the immunisation programme across all regions.
Ensure that front line staff who will deploy the vaccine are healthcare providers and integrated within current healthcare and vaccination systems.
Safety surveillance and reporting
Assess the acceptability of the adverse event profile of the vaccine by healthcare professionals and by the public.
Establish safe vaccination principles.
Ensure adequate tools are available for planning, conducting and reporting pharmacovigilance activities and findings.
Disease burden and characteristics
Evaluate characteristics of the disease relevant for developing an immunisation programme (eg, transmissibility, antigenic variation).
Evaluate the burden of disease in the population.
Mechanism for disease surveillance.
Vaccination equity
Evaluate accessibility and availability of vaccines, and implement strategies to ensure greater reach to, receipt by, under-represented groups.
Determine the ethical considerations of vaccine administration.
Establish a mechanism to facilitate coordination and share data between stakeholders.
Human resources and training of professionals
Establish adequate human resources and financing to provide support.
Training plans in place.
Ensure professional are trained and relevant accreditations are in place.
Ensure support for professionals.
The 38 identified articles were published between 2004 and 2023 (see figure 2A), with (19 out of 38; 50%) published between 2020 and 2022, highlighting the timeliness of this research area. Articles captured research conducted across six continents (Africa, Asia, Australia, Europe, North and South America), and although some of the articles were country-specific (eg, Italy, India and Ghana), several considered vaccine readiness in a global context (13 out of 38; 34%) (online supplemental table S4, column 3). Some articles represented geographical regions or collections of countries (such as the eastern Mediterranean region), while others included research from countries with specific economic characteristics (eg, GAVI-eligible countries; high-income and middle-income countries). Most articles (67%) were created in the context of whether a country is ready to deploy a specific vaccine(s), such as vaccines for the prevention of influenza, meningitis or measles, whereas 33% of articles were not vaccine-specific and considered all vaccine types (see figure 2B).
Across the 38 articles, a variety of methodologies were used to gather information. This included expert review, literature review and policy analysis. In most cases, information was gathered based on expert review (68%). The different approaches used to gather the relevant information, as described in-text by the authors, are summarised in figure 2C. The document types were described within the articles using a range of in-text descriptors, such as a checklist, tools, guidelines or frameworks, as well as more general terms such as ‘factors for consideration’ and ‘recommendations’. Figure 2D shows the different in-text descriptors used to describe each set of guidance documents. The most common type of guidance document was a framework (n=9), followed by guidelines (n=8) but other terminology such as a ‘decision-support platform’ (n=1) was also used.
Common indicators and themes emerged across the different guidance documents
A thematic analysis was conducted to identify common themes that emerged across the different guidance documents. In brief, key factors associated with vaccine readiness were extracted and collated into a comprehensive list so patterns that emerged across different indicators could be evaluated. This facilitated the creation of a final set of 12 distinct overarching themes that are relevant for consideration when assessing whether a country is ready to deploy a new vaccine or improve uptake of underutilised vaccines: sociocultural factors and communication; financing; vaccine characteristics and supply logistics; policy, guidelines and regulations; programme monitoring and evaluation; programme planning; safety surveillance and reporting; sustainable and integrated healthcare provision; disease burden and characteristics; legal, political and professional consensus; human resources and training of professionals; vaccination equity. Figure 3 summarises the core themes that emerged and ranks each theme according to the number of articles where each topic was discussed. A summary description of each of the 12 themes is given in table 1 and the subthemes that emerged within each theme are given in box 1.
Discussion
A scoping review was conducted to identify articles that have been created to help establish whether a country is ready to deploy a new vaccine or improve uptake of an underutilised vaccine. The review identified several common themes and subthemes that consistently emerged across articles, despite the breadth of source materials considered, in terms of the geographical locations, types of vaccines and target populations. This led to the development of 12 overarching themes, which each contained multiple subthemes, reflecting the scope of each topic. Only two articles included topics that were relevant to all the themes identified in this scoping review.30 38
Sociocultural factors and communication emerged as the most prominent theme across the guidance documents. Although this does not necessarily suggest that this theme holds the greatest importance, this highlights the view that engaging the public and having culturally informed communication plans (including resources available in relevant languages and front-line translation services where applicable) in place are critical to the success of immunisation programmes, as well as the acceptance and uptake of vaccines. This aligns with the concept that vaccine hesitancy is context- and culturally-specific and interventions must be tailored for the target audience to elicit an impact.60 The frequency in which sociocultural and communication factors were raised, and depth to which they were discussed, generally increased with time. This may simply suggest that this theme has become a more topical issue with time with an increasingly high research interest globally, but this may also reflect an increased appreciation of the importance of this topic and the current status quo, where communities expect to be carefully and appropriately informed about public health interventions. Given the public focus on COVID-19 immunisation programmes during the pandemic, and the likely corresponding increase in general vaccine awareness and hesitancy, the importance of developing community-informed communication strategies has become a prominent factor in guidance documents. It is apparent that, even if the practical aspects related to vaccine supply, infrastructure and financing are in place, clear communication strategies and tailored public engagement are essential for vaccine deployment success. The WHO Risk Communication Engagement Tool54 highlights the importance of this; the associated guidance documents focus on how to engage the public and generate trust and transparency in the context of immunisation programmes. Negative press and misinformation related to vaccine use can affect vaccine uptake.61 As such, countering this with trustworthy information presented accurately, empathetically and with integrity, is critical and it is equally critical that consistent messages are communicated by diverse and trusted messengers. This is particularly important during the programme implementation phase to prevent the spread of misinformation and maintain engagement with the public using culturally appropriate and regionally specific strategies.62–64 Although not identified in this report as a specific subtheme within the theme of sociocultural factors and communication, the WHO has highlighted gender-related barriers are a key issue impacting the reach of immunisation programmes.65 This indicates that women should play a central role in vaccine deployment, and that this is an important concept that should be considered from a social and cultural perspective when assessing a country’s readiness to deploy a new or underutilised vaccine. It may be critical to ensure that a proposed immunisation programme includes focus on establishing female vaccinators, healthcare professionals, advocates and stakeholders, and includes strategies particularly to improve access for women; in order to broaden accessibility, adjust social and cultural expectations and address gender-related barriers.66
The importance of adequate and sustainable finance being in place to initiate and maintain immunisation programmes has been highlighted in this scoping review. Many articles recognised that financial and economic factors underpin our ability to facilitate actions required to successfully roll-out a new vaccine or improve uptake of an underutilised vaccine. This draws attention to the high degree of interdependence across themes. Taking action to improve communication strategies, train personnel, organise adequate transport and waste management systems requires funding, which is in turn dependent on political will. The tremendous impact that organisations, such as the Global Vaccine Alliance (Gavi), have had on protecting people’s health by increasing equitable and sustainable use of vaccines, in part through the provision of financial support, is well recognised.67 Another key factor that emerged was the importance of considering vaccination equity within a country from the outset. A systematic review of the uptake of the measles, mumps and rubella (MMR) vaccine in Europe found associations between ethnicity, low income and education levels with lower MMR vaccine uptake.68 However, in lower-income countries, other indicators such as gender and number of children, maternal age, and religious beliefs, are indicators of vaccine uptake. Lower educational level and lower income of a child’s caregiver are also related to lower vaccine uptake.69–71 Ensuring that equity is considered from the outset requires proactive measures to be in place to actively evaluate factors, such as accessibility and vaccine distribution, before vaccine deployment.72 73 This theme frequently emerged across guidance documents, where there was often a focus on reaching vulnerable populations, such as children,57 pregnant women35 and older adults.48 Although vaccination equity is recognised as an important aspect for consideration when deploying new vaccines or improving the uptake of underutilised vaccines, specific systems and processes for establishing equity are often not readily available.74 While the importance of vaccination equity is well recognised, this knowledge does not necessarily translate into practical steps to ensure that people who are underserved by immunisation programmes are adequately provided for. The subthemes identified in this scoping review that address vaccination equity lack detail compared with other topics, such as ‘Vaccine Characteristics and Logistics’. Guidance with clear methods and systematic approaches to ensure vaccination equity in global and regional contexts is needed to improve application of this critical component of all immunisation programmes.
In the modern era, the occurrence of the COVID-19 pandemic was a watershed moment for exploring readiness to deploy new vaccines. This led to a substantial increase in the number of guidance documents that have been created to support the introduction of vaccines across the globe.13 31 35 46 48 53 75 Unsurprisingly, readiness to deploy COVID-19 vaccines represented a substantial proportion of vaccine-specific work published in the 2020–2022 period. Guidance documents that were written following the COVID-19 pandemic, differ substantially from previous documents, in terms of the level of detail provided and the specificity of the recommendations. Guidance has become more focused and action-oriented; for example, the COVID-19 Vaccine Introduction Readiness Assessment Tool 2.011 included regulatory guidance to ensure COVID-19 vaccines can be administered to individuals within specified time frames. In addition, while there was an obvious focus on COVID-19 vaccines during this period, guidance was also more often developed with a view to global applicability, compared with earlier documents focusing on vaccines within a specific country or region.28
This scoping review has several limitations. While common themes and subthemes that occur across various guidance documents have been identified, substantial heterogeneity between document types and intended context of use meant that the terminology within each document is highly variable, and therefore, challenging to synthesise. For example, extracting salient information that was common to both generic global guidance documents and highly specific local, regional documents led to a high degree of heterogeneity in considered advice. As similar topics were often described using different terms, careful judgement was needed when synthesising information to establish whether the articles were focused on similar themes. This was further complicated as the scoping review considered both prospectively created articles and retrospective reflections, such as barriers to successful delivery of immunisation programmes. Importantly, while common themes that emerged were summarised and synthesised, the lack of inclusion of a specific topic (or a less prominent theme or subtheme which was discussed less frequently across articles) does not negate its importance, as these indicators may be of critical importance in some contexts and/or environments. While a careful search strategy was designed and tested using specific search techniques such as text analysers to identify words that occur more than once within a predetermined list of tools, and MeSH tools to identify terms that match titles of the guidance documents, this approach did not identify a range of relevant guidance documents that were later found through reference lists and expert knowledge. Over 6000 articles were identified in the original search strategy, demonstrating the challenge of finding the appropriate level of specificity and sensitivity in the search strategy.
The success of an immunisation programme’s deployment of a new vaccine or efforts to improve uptake of an underutilised vaccine, is critically dependent on the programme’s readiness to do so. While indicators identified in this scoping review have not been shown to be predictive of successful vaccine roll-out, an example of the benefit of having guidance documents in place was elegantly demonstrated by the Ministry of Health and Family Welfare in India.76 Across India, multiple geographical locations were identified as not being ready to deploy routine immunisation schedules, but use of a checklist in each location enabled corrective action to be taken, such that 69% of the locations were eventually considered to be ready to deploy the immunisation schedule.76 It is plausible that the factors identified in this scoping review could be further refined to form the basis of an approach that could be used to assess a county’s readiness to deploy a new or underutilised vaccine. At present, it would not be possible to prioritise or weight different themes across geographical regions and settings without a substantial evidence base. Should this be necessary in the future to further enhance vaccine deployment and assessments of readiness, international, national and regional experts may need to consider context-specific prioritisation/theme weighting or develop a tool in which the end user defines an appropriate weighting system.
Conclusion
A country’s success in supporting new vaccine deployment and vaccine uptake is dependent on the country’s readiness.48 This scoping review has identified numerous guidance documents that aim to identify these factors. Of the 38 texts identified in this review, only 230 38 (which were focused on a specific disease (eg, influenza) or population group (eg, pregnant women), respectively) discussed all 12 overarching themes. Each theme was discussed in at least half of the guidance documents, and we believe all 12 themes are critical for establishing the successful introduction, deployment and administration of new vaccines and to improve underutilised vaccine uptake. As such, a new innovative evidence-based vaccine readiness assessment tool could be developed which comprises the themes and subthemes identified here. If such an approach were adopted, the relevance of these indicators would have to be established through formalised processes, validated by experts and field tested to ensure global applicability outside of a pandemic setting. In summary, this work has identified key themes that emerge across guidance documents that could be used to form the basis of a vaccine readiness assessment tool that could be used globally in preparation for the deployment of any new vaccine or improved vaccine uptake.
Supplemental material
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. The completed data extraction form, which is the source data for results figures and tables, is publicly available on GitHub, along with the code required to generate the results: https://github.com/lukebax/readiness.
Ethics statements
Patient consent for publication
Ethics approval
This systematic review of already published and non-identifiable data was considered exempt from ethics review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RM and RS contributed equally.
Contributors VM: accessed and verified the underlying data, analysed the data and wrote the manuscript. AlB was involved with study conceptualisation and reviewed and edited the manuscript. ALE: reviewed and edited the manuscript. LH: project administration, reviewed and edited the manuscript. NH: reviewed and edited the manuscript. MPC: reviewed and edited the manuscript. LB: reviewed and edited the manuscript, accessed and verified the underlying data, methodology. SV: project administration, supervision, reviewed and edited the manuscript. RM was involved with study conceptualisation and reviewed and edited the manuscript. RS: supervised, drafted, reviewing and edited the manuscript. AoB: accessed and verified the underlying data, methodology, analysed the data, reviewed and edited the manuscript. AoB also acts as guarantor for this article.
Funding This work was supported by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA.
Competing interests LH, AE, AL, RM and AlB are employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA and potentially own stock and/or hold stock options in Merck & Co., Inc., Rahway, NJ, USA.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.