Article Text

Abstract
Introduction Neuropsychiatric symptoms (NPS) are common non-motor symptoms among patients with Parkinson’s disease (PD) and significantly impact their overall quality of life detrimentally. Several studies have reported the clinical effect of acupuncture therapy in treating NPS in PD. Therefore, the objective of this systematic review is to evaluate the potential inclusion of acupuncture therapy as an integral component of complementary treatment for PD with NPS.
Methods and analysis From their inception until 1 December 2023, we will search eight databases, including PubMed, Cochrane Library, Embase, Web of Science, China National Knowledge Infrastructure, China Science Periodical Database, Chinese Citation Database and China Biology Medicine disc for randomised controlled trials examining the effectiveness of acupuncture for PD with NPS. Literature screening and data extraction will be carried out independently by the authors. RevMan V.5.3 software will be used for meta-analysis, while the Cochrane risk-of-bias tool will assess the potential for bias.
Ethics and dissemination This systematic review protocol does not require ethical approval because it does not include private information or data of participants. This article will be published in a peer-reviewed journal.
PROSPERO registration number CRD42022324494
- Parkinson-s disease
- Neurology
- Adult psychiatry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
We will conduct an extensive search strategy across eight databases.
Sham acupuncture will be included in the study design, as it has been suggested that the efficacy of acupuncture may be partly due to a placebo effect.
Given the unique attributes of acupuncture, our investigation will focus exclusively on the therapy itself, while details such as the acupuncturist’s expertise or specific acupuncture points will not be detailed.
The limited existing literature on the topic restricts a comprehensive exploration of the mechanisms underlying acupuncture for Parkinson’s disease with neuropsychiatric symptoms in this paper.
Introduction
Parkinson’s disease (PD) is a prevalent neurodegenerative disorder, generally recognised as a movement disorder. However, non-motor symptoms, especially neuropsychiatric ones, have gained more attention in recent years.1 2 The prevalence of neuropsychiatric symptoms (NPS) among non-motor manifestations has been reported to be as high as 87.5%.3 NPS are primarily classified into affective disorders (such as anxiety, depression, fatigue and apathy), psychotic disorders (including hallucinations, delusions and impulse control disorders) and cognitive dysfunction (ranging from mild cognitive impairment to dementia).3 Mood symptoms, including anxiety, depression and apathy, may precede the onset of motor symptoms by several years. Conversely, other non-motor symptoms, such as impulse control disorders, psychosis and cognitive impairment, exhibit a higher prevalence in the advanced stages of the disease.4 The high incidence and long duration of NPS seriously affect the prognosis and quality of life of PD patients.5
Currently, the pathogenesis of PD and its association with NPS remain unclear, with no specific curative treatments available.6 7 Levodopa replacement therapy remains the cornerstone in PD management8; however, it provides significant short-term improvement in motor symptoms but fails to address neuropsychiatric manifestations or slow down disease progression. In fact, levodopa therapy may even contribute to the development of NPS.9 10 Surgical interventions serve as an effective adjunctive approach to PD; however, their limited availability due to technical constraints, efficacy concerns and high costs restrict their widespread use. Adjusting antiparkinsonian drug dosages or employing antipsychotic medications are common strategies for managing NPS.11 Unfortunately, long-term medication use often leads to numerous adverse effects, necessitating dose reduction or discontinuation.12 13 Kinesitherapy and psychotherapy are two alternative therapies with the potential in treating PD with NPS. Nonetheless, more research is needed to fully understand their efficacy, and significant barriers to admission may restrict their general acceptance and application. Therefore, the search for safer and more effective treatments has become an urgent concern.
Acupuncture, a therapeutic practice deeply rooted in traditional Chinese medicine principles, has been widely used in clinical settings for over three millennia. It is recognised for its straightforward approach, remarkable efficacy and well-established safety profile, contributing to its vast potential applications and significant research implications.14 15 In recent years, multiple meta-analyses have demonstrated acupuncture therapy’s effectiveness in treating psychiatric disorders, providing justification for its application in managing neurodegenerative diseases with NPS.16–18 Additionally, the clinical effect of acupuncture therapy in treating NPS in PD has been reported in several studies. Therefore, our objective is to present medical evidence to evaluate the potential inclusion of acupuncture therapy as an integral component of complementary treatment for PD with NPS.
Methods
Study registration
The protocol was developed following the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols19 and has been registered on PROSPERO (CRD42022370674).
Searching strategy
We plan to search thoroughly and methodically in the China National Knowledge Infrastructure, China Science Periodical Database, Chinese Citation Database, China Biology Medicine disc, EMbase, PubMed, Web of Science and Cochrane Library databases from their inception to 1 December 2023. In order to find as much relevant literature as possible, we will use the following terms to broaden our search: “Parkinson Disease,” “Parkinson’s Disease,” “Idiopathic Parkinson’s Disease,” “Idiopathic Parkinson Disease,” “Lewy Body Parkinson’s Disease,” “Lewy Body Parkinson Disease,” “Primary Parkinsonism,” “Paralysis Agitans,” “Acupuncture,” “Pharmacopuncture,” “Needling,” “Electroacupuncture,” “Auricular acupuncture,” “Plum-blossom needle,” “Randomised controlled trial,” “Controlled clinical trial,” “Clinical trials as topic,” “Placebo.” A Chinese translation of the search keywords will be performed before moving on to the Chinese databases. Table 1 presents the search method that may be used on PubMed and the search strategies of other databases can be found in online supplemental eTables 1–7.
Supplemental material
Search strategy for PubMed
Eligibility criteria
We will consider the types of study, participants, interventions, comparisons, outcomes and study quality. All studies will be strictly screened for inclusion in our systematic review and meta-analysis.
Types of study
Randomised controlled trials (RCTs) reported in English or Chinese.
Types of participants
Patients diagnosed with PD using any recognised diagnostic criteria, such as the UK Parkinson’s Disease Society Brain Bank Criteria,20 Movement Disorder Society (MDS) clinical diagnostic criteria21 and diagnostic criteria for PD in China.22
PD patients diagnosed with accompanying NPS using any recognised assessment tools, such as scales recommended in diagnostic criteria developed in China23–25 and other countries.26–28 Trials including patients diagnosed with PD but not definitively diagnosed with accompanying NPS through scales or other evaluation tools will be excluded.
Types of interventions
Acupuncture is defined as needle insertion at acupuncture points in humans, including manual acupuncture, auricular acupuncture and electroacupuncture. Trials including non-invasive therapies like acupressure or transcutaneous electrical nerve stimulation will be excluded due to potential clinical heterogeneity.
Comparisons
Acupuncture versus placebo acupuncture.
Acupuncture versus standard treatment recommended by guidelines, which includes Western medicine such as antiparkinsonian drugs and antipsychotic drugs, surgical treatments like deep brain stimulation and rehabilitation training such as cognitive training.
Acupuncture versus Chinese medicine.
Acupuncture plus other therapy versus other therapy alone.
Acupuncture plus other therapy versus placebo acupuncture plus other therapy.
Types of outcomes
Main results
Hamilton Anxiety Scale, Hamilton Depression Scale, Hospital Anxiety and Depression Scale, Apathy Scale, Lille Apathy Rating Scale, Parkinson’s Disease Sleep Scale, Parkinson Fatigue Scale 16, Schedule Assessment for Positive Symptoms, Montreal Cognitive Assessment scale, Parkinson’s Disease Cognitive Rating Scale and Neuropsychiatric Inventory.
Secondary results
Evaluation tool of motor and non-motor symptoms and daily living ability in Parkinson’s disease: MDS-Unified Parkinson’s Disease Rating Scale.
Quality of life assessment tools encompass the WHO’s Quality of Life Rating Scale (WHOQOL-100) and the Short-form 36.
Adverse events (such as ecchymoma, nausea or headache).
Data selection
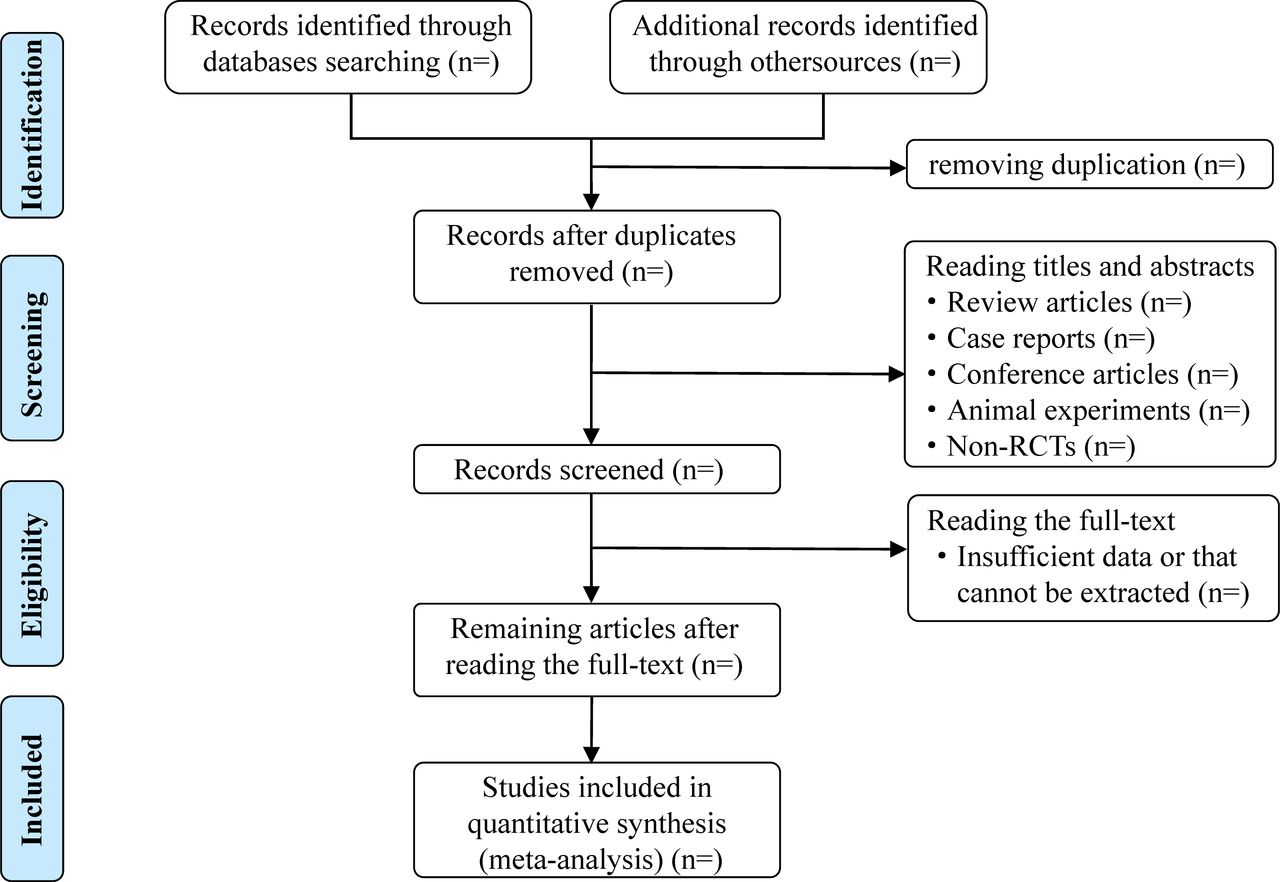
To minimise subjective bias and ensure all prospective RCTs are included, the literature will be independently screened by two investigators. Initially, the literature from each database will be imported into NoteExpress software, where duplicates will be removed. Titles and abstracts of articles published in accordance with predetermined study inclusion and exclusion criteria will be preliminarily evaluated. Eligibility for remaining papers will be determined through a comprehensive full-text review. Selected studies will be exchanged and cross-evaluated by two investigators. Discrepancies will be resolved through consensus or consultation with a third researcher. The rationales and results for study exclusion or inclusion will be documented according to the Preferred Reporting Items for Systematic review and Meta-Analysis flowchart, illustrated in figure 1.

{kind=link}
A Preferred Reporting Items for Systematic review and Meta-Analysis flow diagram of the study selection process.
Data extraction
Information will be collected independently by two reviewers. Extracted data will include basic features of the trial (first author’s name, publication date and study period); baseline patient and disease data (sample size, age, sex, levodopa equivalent daily dosage, disease duration of PD and NPS); interventions (name, treatment course and dose); detailed adverse reactions; and outcome definitions. Exclusions will include (1) non-RCTs, (2) animal experiments, (3) reviews, (4) case reports and (5) studies with incorrect or incomplete data.
Risk of bias assessment
Cochrane’s risk of bias assessment method will be used to evaluate the quality of RCTs, considering the following criteria: random sequence generation, concealment of the allocation sequence, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other sources of bias. Each research domain will be classified into three levels of bias: low risk, high risk and unclear. Studies with more ‘low-risk’ bias ratings will be deemed preferable. Two researchers will independently assess the quality and level of credible research evidence. Any disagreements will be resolved through discussion.
Data synthesis and statistical analysis
Measures of treatment effect
Data will be analysed using Review Manager software (V.5.3). For dichotomous variables, risk ratios will be used to report outcomes. The weighted mean difference will be used for continuous variables assessed with consistent techniques, and standardised mean difference will be used otherwise.
Assessment of heterogeneity
The I 2 and p values will be used to assess heterogeneity among studies. Acceptable heterogeneity is indicated by I 2 ≤ 50% and p ≥ 0.1, and a fixed-effects model will be applied.29 30 Significant heterogeneity is indicated by I 2 > 50% and p < 0.1; in such cases, a random-effects model will be used.29 30
Assessment of reporting biases
When more than 10 articles are analysed, Egger’s test will be used to detect publication bias, with p < 0.05 indicating its presence. If publication bias is identified, the trim-and-fill method will be used to assess its potential impact on the overall findings. Any identified publication bias will be thoroughly examined and discussed in the paper.
Sensitivity analysis and subgroup analysis
When significant heterogeneity is detected in the analysis, we will explore potential sources by conducting sensitivity analysis and subgroup analysis. Moreover, subgroup analyses will be performed based on the following criteria, assuming sufficient data are available:
For patients: type of NPS, severity of NPS, ethnicity, duration of disease, treatment duration and other specific characteristics of the patients such as with or without motor fluctuations, or with or without deep brain stimulation, etc.
For interventions: type of acupuncture and type of comparative group.
Patient and public involvement
None.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors QL and MC originated the research and devised its methodologies. ZP, QL, MC, and WT formulated the search approach. All authors made contributions to the screening of the research articles and assessment of included papers. ML and IIL created the flowchart and processed the data. WT drafted the initial manuscript. LZ supervised the implementation of the entire project.
Funding LZ was the study sponsor. This study was financially supported by the National Natural Science Foundation of China (82174486) and Sanming Project Medicine in shenzhen Nanshan (No. SZSM202103010).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.