Article Text

Abstract
Introduction Familial hypercholesterolaemia (FH) is an autosomal dominant inherited disorder of lipid metabolism and a preventable cause of premature cardiovascular disease. Current detection rates for this highly treatable condition are low. Early detection and management of FH can significantly reduce cardiac morbidity and mortality. This study aims to implement a primary-tertiary shared care model to improve detection rates for FH. The primary objective is to evaluate the implementation of a shared care model and support package for genetic testing of FH. This protocol describes the design and methods used to evaluate the implementation of the shared care model and support package to improve the detection of FH.
Methods and analysis This mixed methods pre-post implementation study design will be used to evaluate increased detection rates for FH in the tertiary and primary care setting. The primary-tertiary shared care model will be implemented at NSW Health Pathology and Sydney Local Health District in NSW, Australia, over a 12-month period. Implementation of the shared care model will be evaluated using a modification of the implementation outcome taxonomy and will focus on the acceptability, evidence of delivery, appropriateness, feasibility, fidelity, implementation cost and timely initiation of the intervention. Quantitative pre-post and qualitative semistructured interview data will be collected. It is anticipated that data relating to at least 62 index patients will be collected over this period and a similar number obtained for the historical group for the quantitative data. We anticipate conducting approximately 20 interviews for the qualitative data.
Ethics and dissemination Ethical approval has been granted by the ethics review committee (Royal Prince Alfred Hospital Zone) of the Sydney Local Health District (Protocol ID: X23-0239). Findings will be disseminated through peer-reviewed publications, conference presentations and an end-of-study research report to stakeholders.
- implementation science
- cardiovascular disease
- genetics
- patient-centered care
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The mixed methods design of our study will form a comprehensive picture of the shared care model benefits and the success of the implementation support package.
We will engage multiple stakeholders to codesign the process and ensure it meets the needs of those who will be impacted most.
By embedding implementation science into the study design, our protocol brings a systematic and evidence-based approach to improving the detection of familial hypercholesterolaemia.
Our observational study design introduces the risk of potential confounding variables influencing our outcomes of interest, which will be considered in any analysis and interpretation of findings.
The 12-month time frame may limit the sample size and exclude patients who decide to undergo cascade testing after the study period.
Introduction
Background
Familial hypercholesterolaemia (FH) is an autosomal dominant genetic condition that causes elevated low-density lipoprotein (LDL)-cholesterol from birth. The cumulative effects of lifelong exposure to elevated LDL-cholesterol can lead to premature atherosclerotic cardiovascular disease (ASCVD) and associated complications.1 2 If left untreated, 50% of men and 60% of women will suffer premature ASCVD before 50 and 60 years, respectively.3 Starting lipid-lowering therapy as early in life as possible can prevent cardiovascular disease and survival can be similar to persons without FH.4 FH is a tier 1 genomic application which means it is a preventable cause of premature cardiovascular disease supported by evidence-based guidelines.5 FH is a significant global health concern estimated to affect 1 in 311 people in the general population.6 Unfortunately, diagnosis rates for FH in most countries are unknown, and most individuals with FH remain undetected and untreated with less than 10% of the estimated 35 million people worldwide with the condition being diagnosed.2 7
The detection and management of FH differs between countries which may be attributed to differences in healthcare system delivery.8 In Australia, detection is primarily driven by opportunistic identification of index cases with some stand-alone programmes for systematic and cascade testing.9 10 A diagnosis of FH can be made using phenotypic criteria and/or genetic testing, the former being largely driven by an elevated LDL-cholesterol level and confirmed using the Dutch Lipid Clinic Network criteria or other internationally used methods.2 5 The proband, or first detected FH case in a family, is referred to as the ‘index’ case. Parents, siblings and children of an index case have a 50% chance of having the condition.11 Genetic testing of first-degree and second-degree relatives of confirmed index cases is referred to as ‘cascade’ testing. Cascade testing is one of the most cost-effective approaches for detecting people with FH as it supports early detection and treatment, thereby reducing the lifelong burden of elevated LDL-cholesterol in both individuals and families.12 However, despite the benefits of cascade testing, uptake remains low in several countries, including Australia, due to barriers associated with direct contact, complex family dynamics and limited practice infrastructure.13 14
Genetic testing allows for a more accurate diagnosis and can open pathways for people to access more suitable treatments, such as proprotein convertase subtilisin/kexin type 9 inhibitors, especially for those that have statin intolerance.11 In 2020, genetic testing for FH was added to the Medicare Benefits Schedule (MBS), which is a list of services subsidised by the Australian government under Medicare, the country’s universal health insurance scheme. However, as of August 2023 only 1886 rebates (1654 for diagnostic and 232 for cascade testing) had been made since the MBS Items were introduced. This equates to less than 2% of the estimated 100 000 individuals in Australia likely to have FH, with only a fraction coming from cascade testing. Explanations for the low utilisation of the MBS Items, particularly for cascade testing, may be due to a general lack of awareness or urgency about FH and the availability of the MBS Items, concerns related to potential exclusions from future insurance coverage of a confirmed genetic diagnosis, and accessibility/waiting times for appointment scheduling.13 Increasing clinician awareness regarding available MBS-funded services and insurance coverage, and reducing wait times through greater general practice involvement in care may address these identified barriers. Increasing detection rates for FH, up to the level of expected cases forecasted when screening was first introduced to the system, would bring substantial individual, community and economic benefits, and have a significant impact on morbidity and death related to ASCVD.
Clinical practice guidelines outline the best available evidence for the delivery of healthcare and include not only what care should be delivered, but how best to deliver that care.15 Although there are well-established guidelines for the care of FH, the ideal model of care for diagnosing and managing FH in Australia has not yet been established. FH is too common to rely on tertiary referral centres to manage all patients, especially for those with only routine management needs. Almost 90% of Australians visit their general practitioner (GP) at least once a year, making this a valuable setting to help diagnose and manage individuals with FH.16 Most tests (90%) for LDL-cholesterol are ordered by GPs, further supporting the benefits of screening and diagnosing patients who may have FH.10 Preliminary feedback from stakeholder interviews conducted by this research team suggests GPs could successfully be engaged in a shared care model, provided that sufficient and appropriate supports are in place.13 GPs can play an important role in increasing the detection of FH with support from tertiary centres for central coordination to facilitate the process. Overall, the primary care setting provides an opportunity to identify and manage more patients with FH.
It is important to develop implementation strategies to effectively create and operationalise new models of care for the translation of FH clinical practice guidelines into practical application.17 Furthermore, models of care should be adaptable to suit local needs and be acceptable to patient and provider.5 18 Implementation science is the study of methods to improve the systematic update of evidence-based guidelines into routine practice and is an essential approach to implementing FH models of care.8 19 There is a clear gap between evidence and practice in the identification and management of FH, including the underutilisation of genetic testing and family cascade testing.17 Barriers include a lack of awareness and understanding of FH among many healthcare providers including cardiologists and GPs.20 Implementation science can help bridge these gaps through well-designed research protocols that use strategies such as providing education and resources to support implementation.18 21 Implementation science frameworks help to understand the underlying contextual factors that may impact the success of an intervention, thereby helping to identify appropriate strategies to address those barriers.15 Our study will provide evidence to support the successful implementation of a model of care to improve the detection and management of FH into routine practice across primary and tertiary settings. This model of care could then be scaled up to support the timely diagnosis, treatment and management of a range of genetic conditions.
Research question
How can existing tertiary health services support the implementation of a primary-tertiary shared care model to improve detection of FH?
Aim
Our aim is to implement a primary-tertiary shared care model to improve the detection of FH in New South Wales (NSW), Australia.
Objectives
The primary objective of this study is to evaluate the implementation of a shared care model and support package for genetic testing of FH. The secondary objective is to evaluate the patient experience of the shared care model.
Methods
Study design
The approach to implement the primary-tertiary shared care model has been guided by the Exploration, Preparation, Implementation, Sustainment (EPIS) framework.22 The EPIS framework guides projects through key stages of the implementation process and highlights important factors influencing implementation success with the broader ‘outer context’ (system) and proximal ‘inner context’ (organisation) across each EPIS stage. The exploration and preparation stages have been conducted by this research team and involved identifying barriers and enablers to implementation of the shared care model (ie, exploration), followed by tailoring the shared care model and implementation supports to local needs (ie, preparation). The third phase (ie, implementation) of the study will use a mixed methods pre-post implementation study design conducted over a 12-month period.23 A combination of quantitative (ie, surveys and patient data) and qualitative (ie, semistructured interviews) outcome measures will be collected. Using this design, the impact of the primary-tertiary shared care model for FH will be compared against a historical usual care model for FH. The mix of quantitative and qualitative outcome measures will help form a comprehensive picture of the shared care model and the success of implementation supports tailored to match the contextual needs of healthcare providers and patients. Additionally, the pre-post study design offers an ideal approach to examining implementation under real-world conditions.
Study setting
The study will be conducted at NSW Health Pathology and Sydney Local Health District through the Vascular Health Clinic at Royal Prince Alfred Hospital (RPAH). The Vascular Health Clinic receives approximately 120 FH testing request referrals per year. NSW Health Pathology employs over 4000 staff and operates more than 60 laboratories, where it conducts more than 61 million tests per year from 200 pathology collection services in NSW public hospitals and community health facilities. Sydney Local Health District is located in the centre and inner west of Sydney. Around 16 000 staff are employed at Sydney Local Health District, responsible for the health and well-being of more than 700 000 people living locally, and in rural and remote parts of NSW and Australia. There are 577 general practices within the 587 km2 area of the Central and Eastern Sydney region providing services to 1.5 million individuals living in the area.
Eligibility criteria
Healthcare providers
All internal and external healthcare providers associated with the Vascular Health Clinic at RPAH including referring GPs, nurses, physicians (eg, cardiologists, geneticists, pathologists, paediatricians) and genetic counsellors.
Patients
The patient sample will include confirmed index cases and their relatives referred to the Vascular Health Clinic at RPAH in Sydney, Australia. Detailed information on the patient sample can be found in figure 1.

Study protocol flow diagram for evaluating the implementation of the primary-tertiary shared care model. *Cardiologists, geneticists, pathologists and paediatricians. FH, familial hypercholesterolaemia; GP, general practitioner; REDCap, Research Electronic Data Capture; RPAH, Royal Prince Alfred Hospital.
Intervention
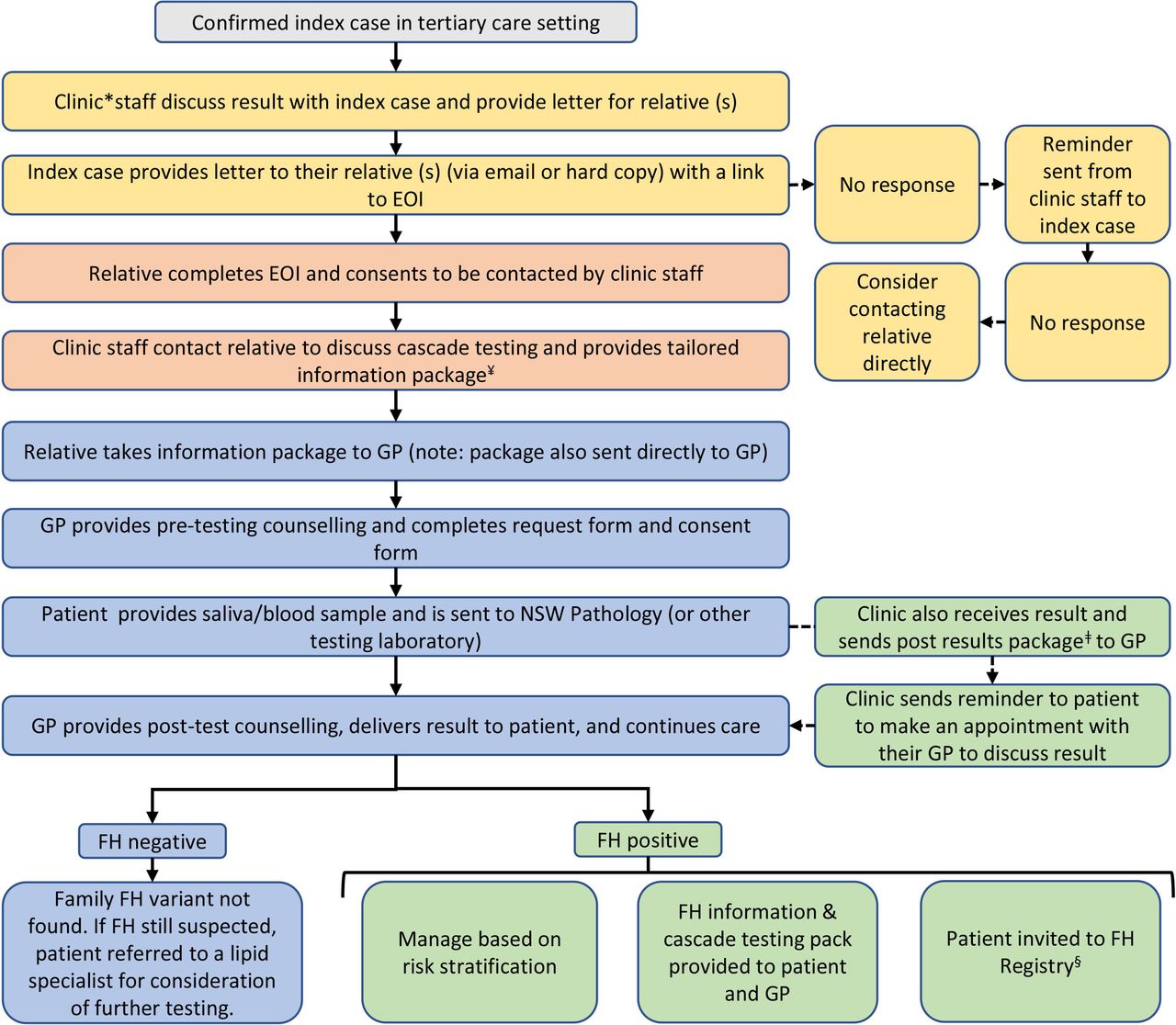
The intervention is described according to the Template for Intervention Description and Replication (TIDieR) guidelines24 (online supplemental appendix 1). The shared care model begins following the diagnosis of a genetically confirmed index case within the Vascular Health Clinic (figure 2). A family letter is provided to the index case to give to their relatives or, if the index case prefers, and with their consent, Vascular Health Clinic staff will contact relative(s) on the index case’s behalf (online supplemental appendix 2). The family letter has been translated into different languages to ensure FH cascade genetic testing is offered to all relatives of index cases. The Research Electronic Data Capture (REDCap) online database will be used to seek an expression of interest (EOI) from the relatives, where they can provide their contact details if they would like to learn more about cascade testing. The family letter includes a URL and a QR code with a link to REDCap and can be sent via email or provided in hard copy. When an EOI form is completed, staff at the Vascular Health Clinic will contact the relative by telephone or email within 1 week and provide more detailed information about cascade testing. If the relative cannot be reached by either telephone or email, clinic staff will make a second attempt to contact them requesting they reach out to the clinic at their convenience. Relatives are then emailed a cascade testing package that includes supporting paperwork to allow consent and ordering of FH cascade genetic testing with their GP. This package is also sent directly to the relatives preferred GP and includes a one-page cascade screening guide for the GP, a prefilled pathology request form, a genetic testing consent form, a list of educational resources and access to additional support through a direct line for GPs to the Vascular Health Clinic (online supplemental appendix 3). Once genetic test results are received by the clinic a post results package is sent to the GP providing guidance on what to do with the results (online supplemental appendix 4). General practice and other specialist engagement with tertiary hospital clinics can be challenging, particularly when pathways for referral are not clear and where referring doctors have had previous negative experiences. To address this, our intervention will focus on promoting respectful, two-way communication of the benefits of early detection and preventive treatment. Additionally, the research team conducted preliminary work with key stakeholders to tailor the shared care model to local needs.13 This includes providing further support through an online health information portal for GPs (ie, HealthPathways), a patient information booklet, a fact sheet on FH with the NSW Centre for Genetics Education and continuous professional development (CPD) opportunities for GPs through an online CPD Journal programme (ie, Medicine Today, a peer-reviewed journal of clinical practice).
Supplemental material
Supplemental material
Supplemental material
Supplemental material

{kind=link}
{kind=link}
FH intervention for the primary-tertiary shared care model. *Refers to Royal Prince Alfred Hospital Vascular Health Clinic. ¥Includes one-page cascade screening guide for GP, prefilled pathology form, genetic testing consent form, patient FH fact sheet and FH-specific resources for primary care. ǂFor positive results, the package includes results letter for GP, results letter for patient, family letter and FH registry consent form. §The National FH Registry is an electronic database where patients can provide consent for their medical information, family history and other related information to be collected for research purposes. EOI, expression of interest; FH, familial hypercholesterolaemia; GP, general practitioner; REDCap, Research Electronic Data Capture.
Recruitment
Quantitative surveys
Healthcare providers will be recruited via an email sent to a purposive sample of key stakeholders associated with the Vascular Health Clinic at RPAH, containing a link to the online REDCap form where they will be asked to complete the implementation outcomes survey.25 The recruitment of healthcare providers will take an arms-length approach whereby initial contact will be made by an investigator with legitimate access to potential participants’ contact details but is not in an unequal workplace relationship with potential participants. The investigator will approach the healthcare provider by email invitation to request their participation in the study, indicating that they have been identified as a key stakeholder involved in implementing the primary-tertiary shared care model.
Patients referred to the Vascular Health Clinic will be identified by the clinic staff and invited to participate in the study by email. The email will be sent by the patients’ physician or a member of their treating team and will include a link to REDCap where they will be asked to complete the patient-reported experience measure (PREM).
Semistructured interviews
At the end of the survey, participants will be asked if they would like to participate in an interview to explore, in more detail, their experience and/or thoughts on the shared care model.
A flow diagram for the study protocol is presented in figure 1.
Outcomes
Primary outcomes
The evaluation of the shared care model implementation will be guided by a modified implementation outcome taxonomy.26 27 Implementation outcomes are conceptually different from health service and clinical effectiveness outcomes. The implementation outcome taxonomy distinguishes between three inter-related types of outcomes: implementation/process, health service and patient health. While the end goal is improvements in health service and patient outcomes, implementation/process outcomes precede these, with the latter outcomes being impacted by changes in implementation processes (ie, changes in clinical practice to deliver the intervention). A summary of primary outcome measures is presented in table 1.
Summary of primary outcome measures
Secondary outcomes
Patient experience will be captured using a PREM during the 12-month implementation period. PREMs are routine state-wide surveys used to gather patient feedback across all levels of the health system to improve patient care.
Outcomes will compare the impact of the new shared care model over a 12-month period against a historical usual care control condition.
Quantitative outcome data
Quantitative pre-post data will be collected from TrakGene, a clinical genetics database, and routine electronic medical record data collected at RPAH.28 29 Quantitative outcome data will be collected through surveys (ie, using REDCap) sent to providers and patients. The surveys will be administered at a single time point and will take approximately 5 min to complete.
Qualitative outcome data
Semistructured interviews will be conducted both during the implementation and at the 12-month follow-up. Semistructured interviews will be conducted online or in person, depending on the participant’s preference. The online semistructured interviews will be conducted via the Zoom or Microsoft Teams videoconference platforms. The interview guide will be informed by the EPIS framework22 and literature on implementing genetic testing in primary care. The interview structure will be guided by the constructivist framework, allowing the conversation to be shaped by feedback from interviewees. The interview will be approximately 60 min in duration.
Implementation cost
A separate protocol is planned for a model-based health economic evaluation to represent the ‘intervention’ and ‘usual care’ comparator cohorts, and their resulting costs and effects.
Planned sample size
For the quantitative data, our statistical power estimation is based on the difference in the rate of cascade tests per index case before and after the adoption of our model. An estimated total sample size of 124 index cases will provide 80% power for a two-sided α=0.05, where there is a rate of 0.30 during the historical control and 0.60 after adoption of the shared care model (calculated using G*Power 3.1.9.7). The RPAH laboratory received 123 FH testing request referrals in 2021, which would provide a sufficient sample if similar numbers were received in 2022–2024.
For qualitative data pertaining to the implementation of the shared care model, we will use the concept of theoretical saturation to determine the interview sample size. From our experience, we anticipate conducting approximately 20 interviews throughout the 12-month study period.
Data analysis
Quantitative data analysis
Quantitative pre-post data and implementation outcome surveys will be analysed using SAS V.9.4 (SAS Institute). Descriptive statistics will be used to summarise demographic data, such as mean and SD, median and IQR, and sample maximum and minimum for continuous data, and frequencies and proportions for categorical data. Statistical significance will be set at p≤0.05. Correlations between the acceptability, appropriateness and feasibility scales will be estimated using Pearson and Spearman rank-order correlation coefficients. Evidence of delivery data will be analysed using a Poisson regression model. Fidelity data will be analysed using logistic regression with potential confounders (eg, age, ethnicity, education level) included in the model. Goodness-of-fit diagnostics will be conducted, and if overdispersion of count data is identified then a negative binomial regression will be used. Timely initiation from referral to genetic testing and diagnosis will be assessed by linear regression.
Qualitative data analysis
Qualitative data will be coded and thematically analysed using QSR NVivo software according to a constructivist framework approach. This approach seeks to understand a social phenomenon and construct theories through participants’ experiences, using iterative data collection and analysis.30 EPIS constructs will be coded in relation to how they influence the implementation outcomes, such as how organisational staffing processes affect the feasibility of the model. Sample sizes provided are estimates, as data collection will continue until thematic saturation is achieved.
Patient and public involvement
Patient and public involvement in the design of this research study commenced before the research grant funding application stage. A range of key stakeholders with policy and practice expertise from NSW, Australia, were consulted to help codesign the shared care model. Essential partners involved in the codevelopment of the protocol included GPs, genetic counsellors, consumers, pathologists, paediatricians, geneticists and policymakers. Patients with lived experience of FH were involved in the design of this study from the initial planning stages and provided their input through focus groups, interviews and participation on the Project Steering Committee. The research question was informed through consultations with key stakeholders whose expertise and experience directly apply to the study protocol. A Project Advisory Group was established with representatives from local networks within the Sydney Local Health District to help design the project, support recruitment, maximise input while minimising participant burden and identify pathways for disseminating research findings.
Ethics and dissemination
This study was approved by the Ethics Review Committee (RPAH Zone) of the Sydney Local Health District (Protocol ID: X23-0239). Findings from this study will be disseminated through peer-reviewed publications, conference presentations and reports for key stakeholders and partners in the field.
Discussion
This study will evaluate a primary-tertiary shared care model for increasing the detection and management of FH. Our study addresses an important gap in the care of people with FH by increasing detection of FH and enhancing access to genetic testing.5 This study embeds implementation science into the design and methods as an important and necessary component to address and overcome barriers to improving the care of FH.8 For an intervention to be successfully implemented and ongoing, it must be acceptable to the end user (ie, those delivering and/or receiving the intervention).15 By interviewing patients and providers, we are addressing this important element by understanding, from the perspective of the end user, why the primary-tertiary shared care model may or may not be successful. Despite the strong evidence base behind FH care, efforts to translate guidelines into practice are often unsuccessful, likely related to a lack of relevant or appropriate implementation strategies.17 31 The design of this study protocol has taken into consideration previously identified barriers and enablers by this research group allowing for the selection of appropriate implementation strategies tailored to local needs.13 A fundamental element of all FH models of care is early detection and initiation of treatment to avoid the lifelong burden of elevated LDL-cholesterol, and engaging with GPs will support this process.8 Usual shared care models typically involve GPs initiating collaboration with lipid specialists by referring individuals with suspected FH for diagnosis and treatment.32 33 In contrast, our primary-tertiary shared care approach represents a departure from usual care whereby the GP is actively approached and supported as an integral component of the model. This unique perspective offers an innovative way of evaluating the approach, underscoring its potential success, particularly when overcoming the initial challenge of promoting genetic testing by GPs. This protocol also incorporates an important aspect of patient-centred care by empowering, and actively involving, index cases as care partners responsible for reaching out to family members for cascade testing. Additionally, it emphasises the importance of establishing linkages and collaboration with primary care providers, contributing to the achievement of integrated and partnered care during the early stages of case management. Successful implementation of our primary-tertiary shared care model will support early detection of FH as cascade testing extends across age groups, in particular children and young adults who have the most to gain from early detection.34
Findings from this study will be reviewed by the research team to identify core elements of the shared care model and implementation supports. Based on these core elements, recommendations will be made to support the long-term sustainment of the shared care model at the local level and broader scaling to other local health districts through the state-wide reach provided by NSW Health Pathology. A scale-up model will be formulated, which will include recommendations for model protocols and knowledge translation resources that could be used across NSW, Australia and internationally. The model has been designed to be incorporated into existing care workflows and make use of available funding reimbursement for genetic testing, enhancing the ability for scale-up to other tertiary hospitals in Australia.
There are some potential limitations to this study. Findings may not be generalisable to other settings due to differences in staff, patient populations, leadership and organisational culture. For example, fidelity could vary based on staff engagement levels with the new model of care. Measures for acceptability, appropriateness and feasibility may be subjective, influenced by providers’ perceptions on how the model fits within their healthcare setting. Qualitative interviews will provide individualised feedback that could vary across settings and patient populations. However, steps will be taken to address these limitations to ensure core elements and implementation supports, and a well-planned implementation handover, are in place to support scale-up and implementation into policy and practice.
Results of this study have significant potential to improve patient and clinical outcomes by identifying and testing family members at risk. Our model will increase capacity building in general practice by supporting GPs to implement genetic medicine as part of standard practice. Long term, this model will lead to the prevention of early-onset coronary artery disease by improving the therapeutic management of FH. Additionally, this project will lead to improvements in patient outcomes through earlier and higher rates of FH detection in the community, facilitating commencement of lipid-lowering therapy, and addressing lifestyle factors to reduce the risk of coronary artery disease.35 36 Our shared care model will enable patients to receive care closer to home, within their communities, and avoid potential long waiting lists. Our shared care model will also support the development of meaningful and equal partnerships between hospital clinics and general practice. As a tier 1 genomic application, FH has strong evidence supporting the use of genetic testing.5 In Australia, cascade screening for FH and treatment with lipid-lowering therapy is a cost-effective means of preventing coronary heart disease in families at risk of FH,37 which underpinned the MBS Items for genetic testing. By frequently engaging with policymakers throughout the planning and development of this project we worked to ensure our model aligns with NSW government strategies and initiatives on genomic medicine.38 39 Acknowledging the dynamic nature of healthcare systems, we recognise that the long-term success of our model hinges on continuous engagement with general practice to understand and address any issues that may impede long-term success. These actions will support and lead the way for introducing genomic medicine into general practice and other disciplines. We anticipate this primary-tertiary shared care model will demonstrate an exemplar approach for integrating genetic medicine into standard care and provide a roadmap for implementation across other genetic conditions.
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge the contributions of Sophie Green and Marie Brigette Cusack who assisted with this project, as well as the project partners NSW Health Pathology, Sydney Local Health District, Central and Eastern Sydney Primary Health Network, NSW Agency for Clinical Innovation, NSW Ministry of Health and the FH Australasia Network and Australian Atherosclerosis Society. The authors also acknowledge research and implementation partners Dr Brendan Goodger, Dr Teresa Anderson, Bridie Carr, Kerrie Martin, Dr Olivia Hibbitt, Professor Gerald Watts, Dr Jing Pang and Dr Ross McLennan.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @KLBirkenhead, @runningdoc14
Contributors The study was conceived by MNS, CT, DS, CS, SS, AP, LE, CMH, GF, SL, MC, ER and RT and all authors contributed to the study design. KB and MNS wrote the initial draft of the manuscript. All authors contributed to and approved the final version of the manuscript.
Funding This work was supported by an NSW Health Translational Research Grant Scheme (H22/4011) and a Heart Foundation Vanguard Grant (105721).
Disclaimer The funding arrangement ensured the funders have not and will not have any role in study design, collection, management, analysis and interpretation of data, drafting of manuscripts and decision to submit for publication.
Competing interests DS has received grants from Regeneron, Amgen, Arrowhead, Ionis and Novartis via Sydney Local Health District; consulting fees and speaker fees from Amgen and Novartis; and drug samples for a treatment adherence programme from Sanofi. CMH has received Amgen, Sanofi and MRFF grants looking at FH identification in the general practice setting, and assisted in the Amgen-funded independent education design for the GP. MNS is supported by an NHMRC Investigator Grant and received honoraria related to consulting, research and/or speaker activities from Amgen.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.