Article Text

Abstract
Purpose Evidence about the associations of migraine features with cardiovascular risk profiles in Chinese population is lacking. The Migraine Exposures and Cardiovascular Health in Hong Kong Chinese Women (MECH-HK) cohort was constructed to investigate longitudinal migraine features and their cardiovascular implications in Hong Kong Chinese women.
Participants We enrolled 4221 Hong Kong Chinese women aged 30 years or above from October 2019 to December 2020. Demographics, reproductive information, lifestyle factors, disease history, blood lipids and glucose, anthropometrics and body compositions were measured during baseline and follow-up. Migraine diagnosis followed the International Classification of Headache Disorders-3 criteria. Migraine features were longitudinally tracked using a migraine diary and summarised by a wide range of epidemiological metrics. Cardiovascular health was assessed using the Framingham risk score (FRS).
Findings to date From October 2021 to June 2023, 3455 women completed the first follow-up measurement. The retention rate was 81.9%. The average age at baseline was 54.40 years. The mean blood glucose, high-density lipoprotein cholesterol and low-density lipoprotein cholesterol levels were 6.44 mmol/L, 65.06 mg/dL and 102.40 mg/dL, respectively. The average FRS was 0.06. Participants had a 10.3% prevalence of migraine or probable migraine. After 1.27 years of follow-up, the median migraine attack frequency was 0.99 attacks/month, with an incidence rate of 2.55 attacks/person-month and a median duration of 7.70 hours/attack. Sleep problems (64.7%) and stress (54.0%) were the top triggers, while prevalent accompanying symptoms were nausea (67.4%), photophobia (39.9%), phonophobia (30.0%) and vomiting (26.2%). Migraine auras included blurred visions (59.6%), flashing lights (41.3%), blind spots (33.0%), pins and needles (6.4%) and halo (1.8%).
Future plans The follow-up for the cohort will be implemented every 2 years. MECH-HK will provide unique longitudinal data on migraine features in Hong Kong women. The linkage between migraine features and cardiovascular disease risk progression will be identified by a long-term observation.
- Migraine
- Cardiovascular Disease
- Epidemiology
Data availability statement
Data are available upon reasonable request. The data used and/or analysed during the current study are available from thecorresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Migraine Exposures and Cardiovascular Health in Hong Kong Chinese Women (MECH-HK) is the first cohort to evaluate the longitudinally migraine features and the cardiovascular disease (CVD) risk links in an Asian population, specifically initiating the first female cohort in Hong Kong.
Migraine features were longitudinally and consecutively recorded by a migraine diary. A wide range of epidemiological metrics were used to describe the migraine features in terms of migraine attack incidence and frequency, attack duration and intensity, and prevalence and reporting rate of specific migraine features.
The establishment of baseline infrastructure and the follow-up lay the groundwork for investigating the impact of migraine and other risk factors on CVD incidence and mortality among Chinese women in Hong Kong.
The brief 1.27 year first follow-up period was the typical limitation. Long-term observation is needed for tracking enough CVD events.
Introduction
Migraine is a debilitating neurological disorder characterised by recurrent headache attacks, affecting approximately 14–15% of individuals worldwide.1 2 Repeated migraine attacks are agony to patients with migraine, severely impair their quality of life and daily functions and lead to a significant loss of work time and reduced performance. According to the Global Burden of Disease Study, migraine is the second leading cause of disability worldwide, accounting for 4.9% of the global burden of disease measured in years lived with disability.3 Although migraine is often not typically regarded by the public as a serious health condition due to its non-fatal and predominantly episodic nature, its substantial public health significance lies in its causal relationships with pain, disability and damaged social and personal life.
Migraine-specific neurovascular dysfunctions have led to speculation that migraine may increase the risk of cardiovascular disease (CVD). Epidemiological studies have consistently revealed a significant association between migraine and an elevated risk of stroke,4 5 myocardial infarction (MI),5 6 overall CVD7 8 and mortality due to CVD.9 However, most of these studies have primarily focused on Western populations. Moreover, these studies lacked comprehensive data on specific migraine features, such as migraine frequency, duration, intensity and their longitudinal, dynamic variations. Understanding these longitudinal migraine features is pivotal for identifying the subgroup of people with migraine at the highest risk of CVD, thereby facilitating more effective, targeted treatments. As such, it is compelling to investigate whether certain longitudinal variations and patterns in migraine features are particularly associated with a higher CVD risk.
In response to this gap in knowledge, the Migraine Exposures and Cardiovascular Health in Hong Kong Chinese Women (MECH-HK) cohort was established. This cohort aims to prospectively collect long-term, longitudinal migraine features and cardiovascular health information among adult Chinese women living in Hong Kong, compare cardiovascular risk between people with and without migraine and examine the contributions of different longitudinal migraine features in the risk of developing CVD. This manuscript provides a comprehensive MECH-HK cohort profile, detailing the cohort methodology, baseline characteristics and reporting on longitudinal migraine features between Janury 2020 and December 2023. The associations between migraine status and longitudinal migraine features and cardiovascular health will be reported in future publications with longer follow-up data.
Cohort description
Study design and setting
MECH-HK is a longitudinal, prospective cohort study targeting adult women in Hong Kong of Han Chinese ethnicity. The inclusion criteria were (1) aged 30 years and above, (2) both parents of Han Chinese descent, (3) residing in Hong Kong, (4) proficient in Chinese or English and (5) agree to provide written consent. The exclusion criteria included (1) mixed genetic background; (2) a clinical diagnosis of CVDs including MI, coronary insufficiency, angina, ischaemic stroke, haemorrhagic stroke, transient ischaemic attack, peripheral artery disease and heart failure; and (3) cognitive disorder, or have any psychiatric disease that cannot provide accurate information.
We employed a multiple sampling framework to identify study participants. First, we invited collaborating organisations and clinics located across various districts in Hong Kong to recruit participants. These organisations included the Family Planning Association of Hong Kong (FPAHK), Hong Kong Federation of Women’s Centres (HKFWC), Huazhou Hometown Association (HHA), Association of Hong Kong Nursing Staff (AHKNS) and the Integrative Health Clinic (IHC) of The Hong Kong Polytechnic University. FPAHK, KFWC and HHA are non-profit organisations in Hong Kong that provide broad spectrum of services tailored to the specific needs of Hong Kong residents. Second, FPAHK randomly invited eligible women using their services to participate in our study. HKFWC, HHA, AHKNS and IHC randomly selected registered members and sent email invitations to these members to participate in the study. Written informed consent was obtained from each eligible woman who agreed to participate in the study. Ethical approval was obtained from the Human Research Ethics Review Committee of the Hong Kong Polytechnic University (Ref.: HSEARS20171229004).
From October 2019 to December 2020, 4656 women were invited for the study. After exclusions (135 declined, 28 were <30 years, 14 had stroke, 12 had MI, 70 failed to provide informed consent and 176 were uncontactable for baseline assessment), 4221 participants were included in this cohort and underwent baseline assessment (online supplemental figure 1).
Supplemental material
Data collection
Data collection included a self-administered questionnaire, anthropometric and body composition measurements and blood tests. Participants with migraine and probable migraine were required to keep a migraine diary, submitting monthly reports to facilitate the longitudinal assess of the migraine features. The collected variables and relevant data sources are summarised in table 1.
Collected variables and relevant data sources in the Migraine Exposures and Cardiovascular Health in Hong Kong Chinese Women cohort
Identification of migraine cases
The migraine diagnostic procedure, shown in online supplemental figure 2, began with a baseline questionnaire asking participants if they had experienced headaches in the past year. Affirmative responses prompted completion of the ID Migraine, a quick and validated screening tool for migraine identification,10 11 while negative ones led to a question about previous doctor-diagnosed migraines. Participants either screening positive in ID Migraine or having a prior diagnosis were considered potential migraine cases. Those with negative ID Migraine results or no prior diagnosis underwent further evaluation for a history of migraine attacks during their lifetime. The specific screening criteria included the presence of symptoms of photophobia, phonophobia, nausea and vomiting during headache episodes, or the manifestation of neurologic symptoms such as visual flashes or pins and needles within an hour preceding the onset of the headache. Individuals who were found to have a history of migraine attacks were also considered as potential migraine cases. A neurologist collaborating with our team conducted telephone interviews with all initially screened potential migraine participants, identifying migraine, probable migraine, non-migraine headache and non-headache groups according to the International Classification of Headache Disorders 3 (ICHD-3).12 Additionally, migraine participants were further sub-classified by the neurologist into those with aura, without aura and with and without aura migraines, following the ICHD-312. Specifically, probable migraine denotes conditions with migraine-like manifestations, but lacking one criterion for definitive diagnosis per the ICHD-312. Migraine with aura is characterised by transient neurological disturbances, such as visual, sensory or language symptoms, which precede the onset of the migraine.12 Migraine without aura presents as a migraine episode without the preliminary neurological symptoms.12 Migraine with and without aura denotes individuals who experience episodes of both types interchangeably.12
Migraine features
Participants diagnosed with migraine and probable migraine were instructed to maintain a migraine diary throughout the study period. This diary was to record specific details for each migraine attack, including (1) the date and duration of the migraine attack (start and end times); (2) the intensity of the headache, rated on a visual scale from 0 to 10; (3) any transient neurological disturbances, such as visual, sensory or language symptoms, that precede the migraine attack (referred to as 'migraine aura' in the text); (4) any accompanying symptoms occurring concurrently with the migraine attack, such as photophobia, phonophobia, nausea and vomiting; (5) any medication to alleviate pain; and (6) potential migraine triggers, such as menstrual, weather variation and stress. Participants with migraine and probable migraine were contacted monthly through WhatsApp and were asked to provide their migraine diary for the preceding month. A wide range of metrics was defined to describe the migraine features in terms of migraine attack frequency and incidence, intensity and duration and prevalence and reporting rate. These metrics were adapted from definitions used in previous migraine studies.12–14 As shown in table 2, for example, migraine attack frequency (MAF) refers to the mean number of migraine attacks per month,12 while migraine attack incidence (MAI) was defined as the mean number of migraine attacks per person each reporting month.13 The metrics were also adjusted—djusted MAF (aMAF) and djusted MAI (aMAI)—to reflect counts exclusively during months with reported migraine attacks (table 2). Furthermore, to quantify migraine triggers, symptoms and auras, the prevalence was calculated as the proportion of participants demonstrating a specific feature, and the reporting rate was defined as the frequency of a specific feature in monthly migraine diary reports14 (table 2).
Definition of metrics of migraine features in the Migraine Exposures and Cardiovascular Health in Hong Kong Chinese Women cohort
Anthropometric and body composition measurement
Height was measured to the nearest 0.1 cm using a stadiometer, and the body weight was measured using the body composition measurement machine (see next paragraph for details) to the nearest decimal place. Waist, hip and thigh circumferences were measured using a non-stretchable tape to the nearest 0.1 cm.
Body composition was measured using the InBody 270 bioelectrical impedance analysis device (InBody Co., Ltd.), a reliable and valid tool highly correlated with the gold-standard dual-energy x-ray absorptiometry.15 This non-invasive, portable analyser uses multiple electrical frequencies to assess parameters like fat mass, lean mass, protein, minerals and basal metabolic rate. Participants stood barefoot with arms at sides on the device, which sent a small current through the body via hand and foot electrodes. The device calculated resistance to this current to estimate body composition. Trained staff performed all measurements, with regular calibration to ensure accuracy.
Conventional cardiovascular risk factors
The conventional cardiovascular risk factors, including hypertension, obesity, smoking, drinking, physical activity, sleep quality and stress, were assessed in this study. Blood pressure was measured using an electronic sphygmomanometer after participants had been seated for at least 15 min. Two consecutive measurements were taken, and the average value was calculated and used as the final blood pressure value. Hypertension was defined as a systolic blood pressure (SBP) of ≥140 mmHg or a diastolic blood pressure (DBP) of ≥90 mmHg according to the 2018 Chinese guidelines for the management of hypertension.16 The participants self-report hypertension diagnosed by the doctor or currently using anti-hypertensive medications were classified as hypertension cases as well. Body mass index (BMI) was calculated by dividing the weight in kilograms by the square of the height in metres. Overall obesity was defined as a BMI of ≥28 kg/m², and central obesity was defined as a waist circumference of ≥80 cm according to the Chinese Obesity and Weight Guidelines.17
The smoking and drinking status of the participants was self-reported through the questionnaire. Participants were asked to indicate whether they were current smokers, former smokers or non-smokers. The smokers were also asked about the age of smoking initiation. Participants were asked to disclose their current drinking habits, including the frequency of alcohol consumption (daily, weekly, monthly, etc.).
Physical Activity Questionnaire-Short Form (IPAQ-SF) was used to assess participants’ physical activity levels. Participants were asked to report the number of days and the amount of time spent in vigorous-intensity, moderate-intensity and walking activities in the past 7 days.18 IPAQ-SF also asked about the time spent sitting during a typical weekday. IPAQ-SF was scored according to its scoring protocol, which assigns metabolic equivalent (MET) values to different activities based on their intensity.18 The total physical activity score was calculated by summing the MET-minutes per week for each activity category,18 and the PA level was classified as high-, moderate and low level accordingly.
Sleep quality was measured by the Chinese version of the Pittsburgh Sleep Quality Index (PSQI).19 A 19-item scale evaluating seven aspects of sleep in the previous month, including duration, disturbance, latency, daytime dysfunction due to sleepiness, efficiency, quality and medication usage. Each component, rated from 0 to 3, contributed to an overall score between 0 and 21, where higher scores denoted poorer sleep quality.19 A PSQI score over 5 suggested poor sleep or insomnia.
Perceived Stress Scale (PSS-14) was used to measure the stress level. The PSS-14 consists of 14 items that ask about the extent to which individuals feel that their lives are unpredictable, uncontrollable and overloaded over the past month.20 Participants were asked to rate each item on a five-point Likert scale, ranging from 0 (never) to 4 (very often).20 The total score ranged from 0 to 56, with higher scores indicating higher levels of perceived stress.20
Blood lipids and glucose
Blood glucose and lipid levels were measured using point-of-care testing devices that required obtaining a small drop of capillary blood through a fingerstick. The ACCU-CHEK Performa device was used to measure blood glucose levels, while the CardioChek PA device was employed to measure total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C) and triglyceride (TG) levels. The ACCU-CHEK Performa has been identified with acceptable precision (coefficient of variation <14%),21 and the CardioChek PA showed a high clinical agreement from 94.6% to 97.7%.22–24 Participants were asked to fast for at least 8 hours before the measurement.
Framingham cardiovascular risk score
The primary outcome of this cohort study was the changes in the risk of CVD measured by the Framingham 10 year general cardiovascular risk score (FRS)25 from the baseline to follow-up. The satisfactory performance of the FRS in Hong Kong Chinese women was recently reported in a population-based cohort study.26 The rationale for selecting the FRS as the outcome measure is its ability to detect of significant changes in cardiovascular risk within a relatively short time frame.27 28 The predictors used for calculating the FRS included age, treated and untreated SBP, current smoking status, diabetes, TC and HDL-C25.
Demographic and other variables
Demographic characteristics (age, marital status, education, etc.), food frequency (fruits, meat, beans, etc.), daily food consumption (fruit, vegetables and protein), reproductive information (menopausal state, age of menopause, hormonal replacement therapy, etc.), chronic disease information (diagnosis, treatment, family history) and fatigue degree were also collected from the self-administered questionnaire (table 1).
Follow-up
The first follow-up for the cohort was initiated in October 2021 and is currently in progress. Follow-up assessments will be conducted every two years, using the same methodology to ensure continuity and consistency in data collection. The cohort will be followed up for at least ten years.
To minimise the impact of dropout during the follow-up period, we have implemented a two-pronged approach. First, we consider participants who miss certain follow-up assessments but return for later ones as successfully followed, recognising that temporary dropout does not necessarily invalidate a participant’s overall contribution.29 30 Second, we have implemented measures to minimise dropout rates, including maintaining regular contact with participants through newsletters, emails and phone calls, collecting and updating comprehensive contact information at each follow-up and providing incentives in the form of supermarket coupons to encourage the completion of follow-up assessments.
Patient and public involvement
Patients or the general public were not involved in the design, conduct, reporting or dissemination plans of this study.
Findings to date
Follow-up status and baseline demographic information
As of June 2023, a total of 3455 participants have successfully completed the follow-up, achieving a retention rate of 81.9% (online supplemental figure 1). Overall, the participants had a mean age of 54.40 years, with approximately one-third achieved a tertiary or higher degree (32.2%) and had a monthly family income of over 40 000 HKD (33.2%). Of the participants, 65.3% were married or cohabitating, and 81.0% lived with their partner, parents or children (table 3). Generally, younger women were more likely to be married or cohabitating; to live with a partner, parents or children; to have higher education and income levels; and to be employed (all p<0.05) (table 3).
Baseline characteristics of the participants in the Migraine Exposures and Cardiovascular Health in Hong Kong Chinese Women cohort
Longitudinal migraine features
Out of all participants, 283 were diagnosed with migraine, 153 with probable migraine and 128 with non-migraine headaches. Regarding the subtype of migraine, 44 were migraine with aura, 156 were migraine without aura and 83 were migraine with and without aura.
Among the participants with migraine, the median of MAF and aMAF were 0.99 attacks/month and 2.26 attacks/month, respectively; MAI and aMAI were 2.55 attacks/person-months and 5.15 attacks/person-months, respectively; the median migraine duration per attack and migraine duration per month were 7.70 hours/attack and 21.11 hours/month, respectively. The median migraine intensity (MI) was 5.25 (table 4). Similar results were observed for the participants with probable migraine (table 4). In stratified analysis by the migraine subtype, participants of migraine with aura experienced significantly shorter duration and less intensity compared with those without aura and those who experienced migraines both with and without aura (all p<0.05) (table 4).
Migraine features of the participants with migraine and probable migraine in the Migraine Exposures and Cardiovascular Health in Hong Kong Chinese Women cohort
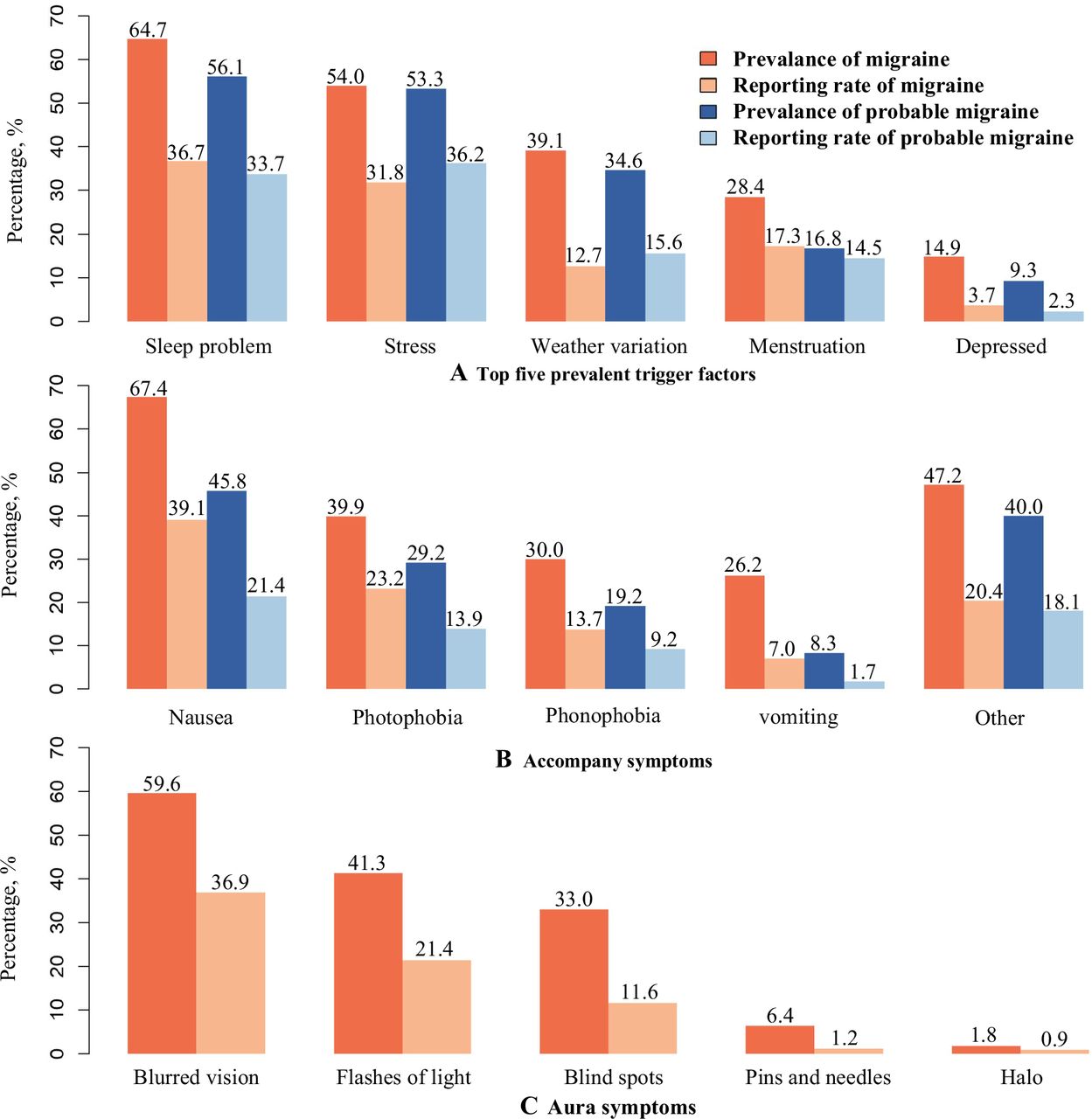
For participants with migraine and probable migraine, the top five prevalent trigger factors were sleep problems, stress, weather variation, menstruation and depression, as depicted in figure 1a. The reporting rate for sleep problems and stress was approximately one-third, while weather variation and menstruation were reported at around one-fourth. Additionally, the reporting rate for depression was less than 4% (figure 1a). In relation to accompanying symptoms among participants with migraine and probable migraine, figure 1b revealed that nausea exhibited the highest prevalence and reporting rate, followed by photophobia, phonophobia and vomiting. Regarding aura symptoms, blurred vision emerges as the most prevalent and frequently reported aura symptom, followed by flashes of light, blind spots, pins and needles and halos (figure 1c).

{kind=link}
Migraine-related characteristics among participants with migraine and probable migraine. Prevalence was calculated by dividing the total number of participants with migraine or probable migraine who demonstrate a specific feature by the total number of participants with migraine or probable migraine. Reporting rate was calculated by dividing the total number of migraine reports that include a specific feature by the total number of migraine reports. Aura symptoms were calculated among the participants with migraine with aura and migraine with and without aura.
Baseline cardiovascular risk profile
Overall, the mean SBP and DBP were 123.68 mmHg and 76.21 mmHg, respectively. The mean BMI, percent of body fat and waist circumference were 23.04 kg/m2, 32.48% and 78.26 cm, respectively. The prevalence rates for hypertension, overall obesity and central obesity were found to be 26.0%, 8.8% and 40.4% respectively. The minority of participants (2.3%) were smokers, while 11.8% of participants were drinkers. Over half of the participants (66.4%) had high physical activity level. Participants had an average PSQI score of 6.2 with 48.9% were suffered from insomnia. The average blood glucose level was 6.44 mmol/L. TC, HDL-C, TG and LDL-C levels were 197.87 mg/dL, 65.06 mg/dL, 158.25 mg/dL and 102.40 mg/dL, respectively. The average PSS-14 score was 24.2. The mean FRS was 0.06. The cardiovascular risk profiles according to three age groups (< 45 years/45–64 years/≥65 years) are shown in table 3. Compared with younger women, older women exhibited higher BMI, waist circumference, percentage of body fat, blood pressure, physical activity, PSS, blood glucose, TG levels and FRS score (all p<0.05). They also showed poorer sleep quality, a lower percentage of smoking and drinking and a higher prevalence of hypertension, diabetes, high cholesterol and central obesity (all p<0.05).
Strengths and limitations
The strengths of our study lie in its unique potential contributions to the field. First, our study is the first to longitudinally observe detailed migraine features and their relationship with CVD risk in an Asian population, addressing a significant research gap. Second, we introduced a comprehensive set of metrics—attack incidence and a nuanced comparison of prevalence with reporting rates—to enhance understanding of migraine phenomena. Third, the rigorously detailed cohort data set a solid groundwork for subsequent investigations into CVD outcomes related to migraines in this population.
Nonetheless, our study was subject to certain limitations. First, despite our sampling framework involving diverse organisations across different districts and randomly selecting participants from their service users and registered members, our study population may not fully represent the entire population of Hong Kong women. Second, the inclusion of only female participants limits the generalisability of our findings to the whole population. Third, the relatively short follow-up period did not allow for an adequate observation of CVD events, thereby precluding their use as the primary outcome of our research at the current stage. Instead, FRS was used. Fourth, recall bias from self-reported questionnaires was an unavoidable concern although its random nature across participants likely did not systematically alter the findings. Lastly, the older age demographic of our study cohort (mean age: 54.4 years) may have contributed to the lower migraine prevalence observed, as migraine prevalence typically peaks between the ages of 35 and 39 years and then decreases after this age range.31 Nevertheless, the age distribution of our cohort aligns with the demographic profile at higher risk for CVD. This ensures that our findings are particularly relevant for this group and supports our focus on investigating the association between migraines and CVD.
Data availability statement
Data are available upon reasonable request. The data used and/or analysed during the current study are available from thecorresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involved human participants and was approved by the Human Subjects Research Ethics Committee at the Hong Kong Polytechnic University (Ref.: HSEARS20171229004) Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to express their sincere gratitude to all women who participated in this study. They would like to extend their heartfelt gratitude to the Family Planning Association of Hong Kong, Hong Kong Federation of Women’s Center, Huazhou Hometown Association, Association of Hong Kong Nursing Staff and the Integrative Health Clinic of The Hong Kong Polytechnic University for their unwavering support and assistance throughout the study. Special appreciation is also expressed to the dedicated research assistants and student helpers for their valuable contributions to the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators Data from the Migraine Exposures and Cardiovascular Health in Hong Kong Chinese Women cohort is open for collaborative research endeavors with non-profit entities. Data access is granted to aid in the advancement of shared scientific interests. Interested parties should contact the corresponding author for further details and to discuss potential collaborative ventures.
Contributors YJX conceived and designed the study and provided administrative, technical or material support to the study; YJX and QY collected the data; QY analysed and interpreted the data and drafted the manuscript; YJX and QS made critical revisions of the manuscript. All authors, including YJX, QY, QS, AYL, CH, HHW, JQ and LY, participated in the planning and reporting the work described in the manuscript. They all read, reviewed and approved the final manuscript. YJX is responsible for the overall content as the guarantor.
Funding This study was supported by the Early Career Scheme, Research Grants Council of the University Grants Committee: HK (grant number: 25101418) and Central Research Grant of the Hong Kong Polytechnic University (grant number: P0009671). The funder had no role in the design, data collection, data analysis and reporting of this study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.