Article Text

Abstract
Objectives The Awareness, Care and Treatment In Obesity maNagement (ACTION) Teens study explored attitudes, behaviours, perceptions and barriers regarding effective obesity care among adolescents living with obesity (ALwO), caregivers and healthcare professionals (HCPs).
Design Cross-sectional online survey study.
Setting Study across 10 countries; here, we report data from UK respondents.
Participants Overall, 416 ALwO (aged 12 to <18 years; body mass index ≥95th percentile for age and sex (WHO charts)), 498 caregivers and 250 HCPs in the UK completed the survey (August–December 2021).
Primary and secondary outcome measures Survey questions addressed key aspects of obesity management for ALwO.
Results Overall, 46% of ALwO perceived their weight as normal or below normal and 86% believed their health was at least good; 56% and 93% of caregivers responded similarly for their ALwO. Despite this, most ALwO (57%) had attempted to lose weight in the past year and 34% felt highly motivated to lose weight. YouTube and social media were most often used by ALwO for information about weight management (41% and 39%); few ALwO and caregivers sought information from a doctor (13% and 22%). Among ALwO who had discussed weight with an HCP (n=122), 49% trusted their weight-management advice. Only 10% of ALwO and 8% of caregivers were told by a doctor that they/their child had obesity. For HCPs, obesity-related comorbidities were the most common reason for initiating weight conversations with ALwO (73%), while short appointment times were the most common barrier (46%). Overall, 30% of ALwO and 11% of caregivers did not feel comfortable bringing up weight with an HCP.
Conclusions Improved education and communication are needed among ALwO, caregivers and HCPs in the UK to help improve awareness of obesity, its aetiology and its impact on health, and to support HCPs to proactively initiate weight-related conversations and build trust with ALwO and caregivers.
Trial registration number NCT05013359.
- nutrition & dietetics
- paediatric endocrinology
- public health
- community child health
Data availability statement
Data may be obtained from a third party and are not publicly available. Data will be shared with bona fide researchers submitting a research proposal approved by the independent review board. Individual participant data will be shared in data sets in a deidentified and anonymised format. Data will be made available after research completion. Information about data access request proposals can be found at novonordisk-trials.com.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Three key stakeholder groups were surveyed: adolescents living with obesity, caregivers and healthcare professionals.
Stratified sampling and demographic weighting of caregivers mitigated selection bias.
Due to the survey-based design, body mass index was calculated using self-reported height and weight data.
The cross-sectional design may have limited the ability to determine cause and effect.
Surveys were hosted online in English; therefore, respondents without internet access or who were unable to read English were, by default, excluded.
Introduction
The prevalence of obesity has risen in young people throughout the UK.1 Data from the 2021/2022 National Child Measurement Programme showed that in England, 10% of children aged 4–5 years were living with obesity and 12% were living with overweight.2 In the same year, 23% of those aged 10–11 years were living with obesity and 14% with overweight.2 Across the UK, disparities in the prevalence of obesity also exist, with those living in more deprived areas facing a greater likelihood of developing obesity than those living in less deprived areas.2 3
Children/adolescents living with obesity (ALwO) are five times more likely to be living with obesity in adulthood than children/adolescents without obesity and have an increased risk of health complications (including cardiovascular and metabolic disease) in adulthood.4–6 Obesity is also associated with mental health issues among ALwO,7 8 and there is increasing evidence suggesting a bidirectional relationship between the two.9–11 Furthermore, socioeconomic disadvantage may increase the risk of comorbidity between obesity and poor mental health, and this risk increases with age.9 However, intervention during early childhood can lead to long-term improvements in body mass index (BMI).12
Lifestyle and behaviour interventions are the cornerstones of treatment for ALwO, and there is a growing body of literature on the effectiveness of multidisciplinary team intervention.13 The National Institute for Health and Care Excellence recognises, among others, the role of primary care providers—often perceived as ‘gatekeepers’—in managing obesity among children/adolescents, including by raising awareness and making referrals to weight-management services.14 15 However, it is unclear how many young people are currently seen specifically for obesity in primary care,16 and available data in England suggest less than one fifth of children with obesity discuss obesity during primary care consultations.17 Furthermore, there is no nationwide requirement to commission weight-management services for young people, and when provided, these services may be variable and fragmented, resulting in geographical inequalities in weight-management services.18 Recently, a pilot scheme of Complications from Excess Weight clinics began in England, in order to deliver on the long-term plan for the National Health Service (NHS), which envisages a holistic, multidisciplinary approach for treating severe obesity-related complications in young people.19 However, this expansion of services is unlikely to reach most young people requiring treatment.18
Obesity in young people is one of the biggest public health challenges in the UK.20 Despite the rising prevalence and current healthcare environment,1 research on lived experiences, needs and challenges regarding obesity management among ALwO, caregivers and healthcare professionals (HCPs) is lacking. The Awareness, Care and Treatment In Obesity maNagement (ACTION) Teens Study explored attitudes, behaviours, perceptions and barriers regarding effective obesity care among ALwO, caregivers and HCPs from 10 countries. Findings from the global, Spanish, Italian and Saudi Arabian analyses have been reported previously.21–24 Here, we present UK data.
Methods
Study design and participants
ACTION Teens (NCT05013359) was a cross-sectional survey study conducted in Australia, Colombia, Italy, Mexico, Saudi Arabia, South Korea, Spain, Taiwan, Turkey and the UK; the full methods have been published previously.21 Data from the UK were collected between August 2021 and December 2021 via an online survey.
Eligible adolescents were aged 12 to <18 years, living in the UK and had a BMI—calculated from self-reported weight, height, age and sex—≥95th percentile for age and sex based on WHO charts.25 Eligible caregivers were ≥25 years of age, lived with their ALwO for ≥50% of the time, were based in the UK and were involved in healthcare decisions for their adolescent. Eligible HCPs were physicians practising in the UK, had worked in clinical practice for ≥2 years, cared directly for patients for ≥50% of their time and were visited by ≥10 ALwO in a standard month. HCPs included primary care practitioners, general paediatricians and those with other relevant specialties (nutrition specialists, paediatric endocrinologists, paediatric gastroenterologists, obstetricians and gynaecologists).
Survey development
Separate yet overlapping surveys were created for the ALwO, caregivers and HCPs. An international steering committee that included content experts, as well as HCPs, developed/approved the survey materials; the members of the steering committee authored the global ACTION Teens Study manuscript, in which the full surveys were published.21
Patient and public involvement
A person living with obesity was involved in the design and dissemination plans for the ACTION Teens Study.
Procedures
KJT Group, Rochester, New York, USA, carried out data collection. Data were collected via an online survey that was programmed with Decipher Survey Software (Forsta). Online panels/databases were used to recruit caregivers and ALwO by targeting/screening adults from a stratified general population sample to identify caregivers of ALwO. The screening forms are available alongside the full surveys.21 Eligible caregivers were invited to participate in the study and were asked to consent to their ALwO’s participation. After recruitment of ‘matched pairs’ of caregivers and ALwO reached a maximum, recruitment continued with a view to increasing the number of respondents to meet the target sample size. Physician panels/databases (online) were used for recruiting HCPs. All surveys were provided in English. ALwO and caregivers received nominal honoraria/panel credit from the online panel company, and HCPs were compensated at fair market value for the UK and their specialty type.
Outcomes
As previously described,21 the surveys investigated key aspects of obesity management for ALwO, including: attitudes towards obesity/people living with obesity and beliefs regarding the impact that obesity has; weight-loss efforts in the past year, motivations/barriers for weight-loss efforts and how successful weight loss/management is defined; history/frequency of discussions about weight and initiator of/responsibility for starting weight discussions between caregivers/ALwO and HCPs; interactions between ALwO, caregivers and HCPs, reasons why obesity might not be talked about and frequency of obesity diagnosis and follow-up appointments; and information sources used to learn about weight loss, weight management, obesity and healthy lifestyles. These outcomes were assessed using Likert scales, numeric responses, no/yes responses or multiple/single item selection (response options dependant on question). To ensure there were no missing responses, participants were required to answer all survey questions.
Sample size
The target sample size for the UK was 675 completed surveys from ALwO, 675 from caregivers and 250 from HCPs. Sample sizes were chosen based on the population size of ALwO in the UK and to balance recruitment feasibility and statistical power. They were designed to achieve a margin of error (around a proportion estimate of 50%) of 3.8% for ALwO, 3.8% for caregivers and 6.2% for HCPs. The margin of error was calculated from a standard normal (Z-) distribution with z=1.96 or approximately 95% confidence.
Statistical analysis
The full analysis set comprised all ALwO, caregivers and HCPs who completed the survey. Deidentified data were analysed by KJT Group using Stata (StataCorp LLC, V.IC 14.2), Excel (Microsoft 365) and SPSS (IBM, V.23.0). Data were described using univariate descriptive statistics (proportions, means and medians). If appropriate, continuous variable outliers (data points two SD from the mean) were removed from the data set when analysing the relevant variable, to control for potential error/misinterpretation that may impact descriptive statistics; therefore, the relevant results were based on a reduced base size. Data for caregivers were weighted based on representative demographic targets within the UK (for sex, age, education, household income and region) for generalisability and to mitigate selection bias. The full statistical methods have been published previously.21
Results
Demographics and characteristics
A total of 416 ALwO, 498 caregivers and 250 HCPs completed the survey in the UK, representing 36%, 43% and 22% of all UK respondents, respectively (online supplemental figure 1). The demographics and characteristics of respondents are summarised in table 1. Most participants were from England. Among ALwO and caregivers, there were more female respondents than male respondents; 30% of ALwO were living with class III obesity and over a third of caregivers had obesity (class I, II or III) (table 1). Most HCPs (60%) were primary care practitioners and 26% of HCPs reported receiving advanced training in weight management or obesity following medical school.
Supplemental material
Demographics and characteristics
Perceptions of obesity
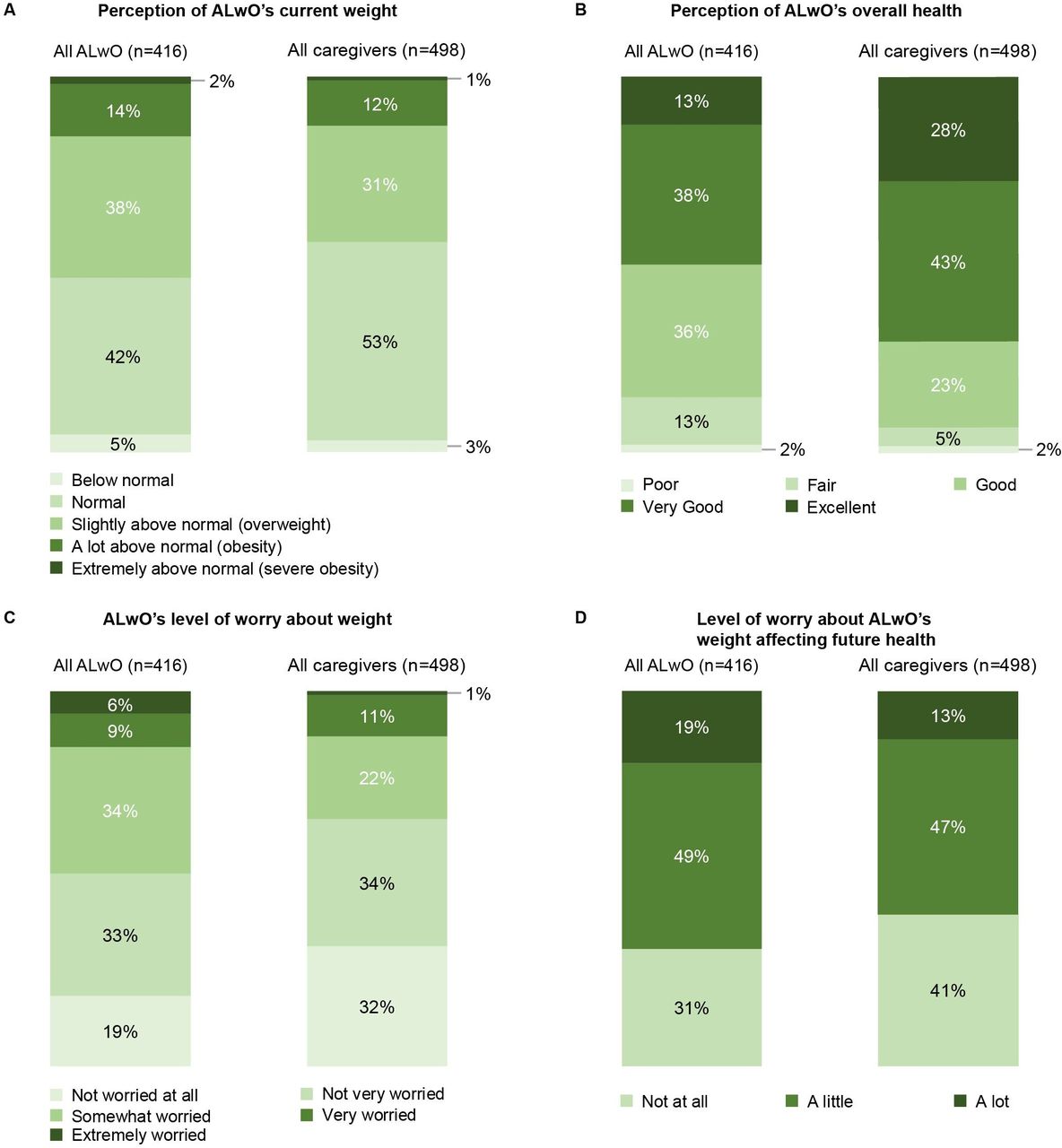
Among ALwO, 46% perceived their weight as either normal or below normal, 86% believed their health was at least good and 50% believed their health was at least very good (figure 1A,B). Similarly, most caregivers (56%) perceived their ALwO’s weight as either normal or below normal, 93% believed their ALwO’s health was at least good and 71% believed their ALwO’s health was at least very good (figure 1A,B).

Participantss responses for (A) perceptions of ALwO’s current weight; (B) perceptions of ALwO’s overall health; (C) ALwO’s worry about weight; (D) worry about ALwO’s weight affecting future health. Data are the proportions of respondents who chose each prespecified option, among all UK ALwO (left bars) or UK caregivers (right bars). Numbers may not sum to 100% due to rounding. ALwO, adolescents living with obesity. Figure adapted from Mears et al.18
Few ALwO (15%) were extremely or very worried about their weight, and a similar proportion of caregivers (12%) believed this to be the case for their child (figure 1C). Less than one fifth of ALwO (19%) and only 13% of caregivers worried a lot about how their/their child’s weight could impact their future health (figure 1D). Among ALwO and caregivers, 31% and 41%, respectively, were not worried at all about the impact of the their/their child's weight on their future health (figure 1D).
Weight-loss attempts, barriers, motivators and attitudes
Overall, 57% of ALwO had made at least one weight-loss attempt in the past year and 28% reported being very likely to make a weight-loss attempt within 6 months; fewer caregivers reported these responses for their ALwO (27% and 20%, respectively).
Lack of motivation was the barrier to weight loss most often reported by ALwO (selected by 46%), whereas caregivers most often reported that none of the specified response options were keeping their child from losing weight (online supplemental figure 2A). ALwO and caregivers also reported barriers related to the cost (selected by 17% of ALwO and 10% of caregivers) and availability (selected by 20% of ALwO and 5% of caregivers) of healthy food and the cost of weight-management programmes (selected by 11% of ALwO and 5% of caregivers). For HCPs, 94% agreed that both unhealthy eating habits and lack of exercise were barriers to their adolescent patients losing weight (online supplemental figure 2B). ALwO’s top motivators for losing weight were wanting to be more confident/feel better about themselves (selected by 50%) and wanting to be fitter/in better shape (selected by 44%); 20% of ALwO had no desire to lose weight (online supplemental figure 3). These data differed to those for caregivers and HCPs: caregivers most commonly believed their child had no desire to lose weight (selected by 35%) and HCPs believed wanting to be more confident/improve self-esteem, wanting to improve social life and wanting to look like peers were the top motivators for ALwO (selected by 70%, 69% and 66%, respectively) (online supplemental figure 3).
Regarding attitudes towards weight loss, approximately one-third (34%) of ALwO felt highly motivated to lose weight and three-quarters of ALwO (75%) felt weight loss was completely their responsibility. In comparison, 45% of caregivers and 55% of HCPs disagreed that weight loss was completely the ALwO’s responsibility. More than half of caregivers (58%) thought their child would naturally slim down as they got older and taller, and 45% felt that following a successful weight-loss attempt, it would be easy for their child to keep the weight off; 21% and 35% of HCPs, respectively, responded similarly for their adolescent patients.
Information sources
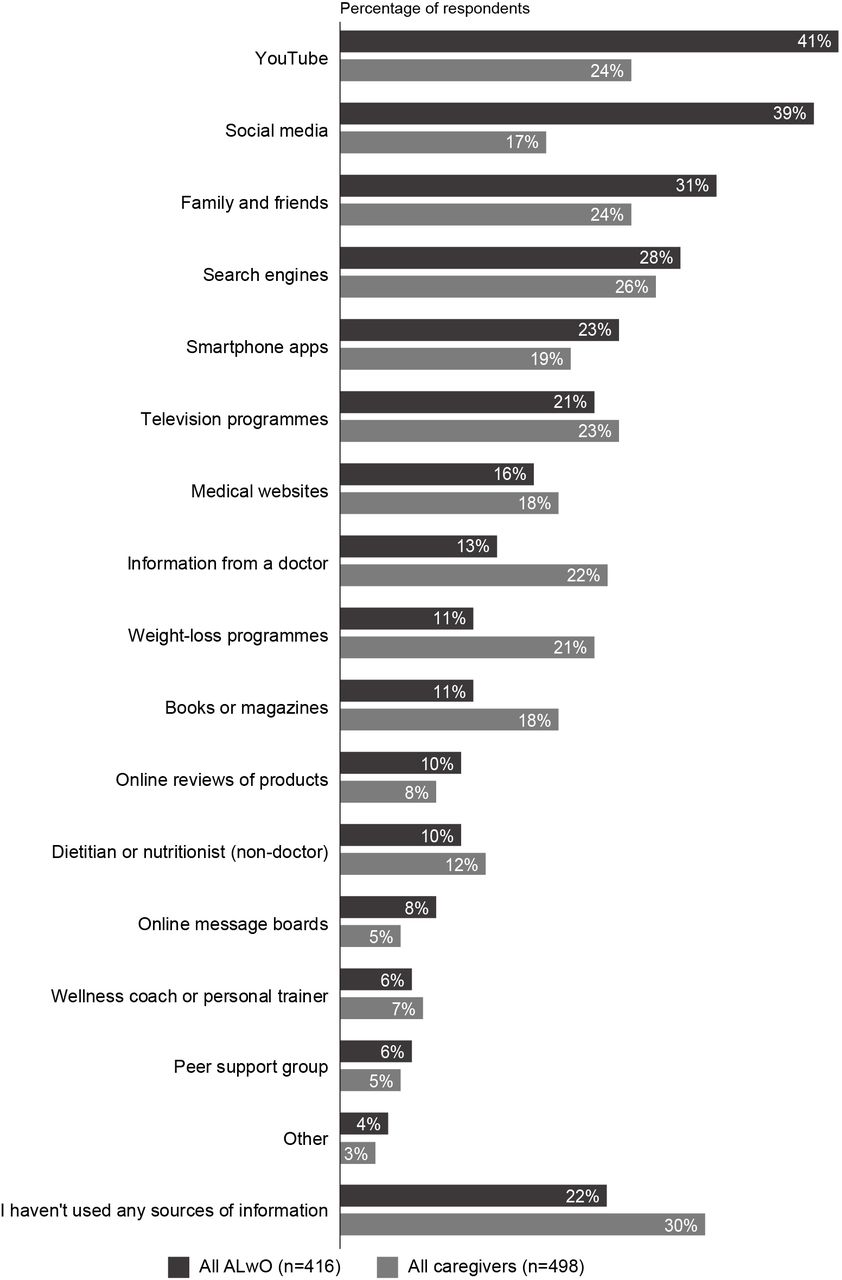
ALwO most often reported that they seek information about weight management from YouTube (41%) and social media (39%); caregivers often used YouTube as well (24%), alongside search engines (26%) and family and friends (24%) (figure 2). Few ALwO (13%) and caregivers (22%) sought information from a doctor.

Information sources used by ALwO and caregivers to learn about healthy lifestyles, weight loss and weight management. Data are the proportions of respondents who reported having used each information source, among all UK ALwO (top bars) and UK caregivers (bottom bars). ALwO, adolescents living with obesity. Figure adapted from Mears et al.18
Conversations about weight
A small proportion of adolescents (10%) and caregivers (8%) had been informed by a doctor that they or their child were living with obesity. Among ALwO and caregivers who had discussed weight with an HCP (n=122 and n=192, respectively) and among HCPs, all groups most frequently reported bringing up the topic of weight themselves during HCP appointments (44%, 41% and 49%, respectively) (online supplemental figure 4A). Additionally, among all ALwO and caregivers, most ALwO (63%) felt they were responsible for initiating weight discussions with an HCP; 43% of caregivers thought that their child should bring it up (online supplemental figure 4B). Concerningly, most HCPs (66%) felt responsibility varied depending on the patient and 7% thought it was the adolescent’s responsibility to initiate weight discussions; only a minority felt it was their own responsibility (18%) (online supplemental figure 4B). HCPs reported the presence of obesity-related comorbidities (73%), the adolescent patient’s weight (64%) and the patient’s mental/emotional state (64%) as the most common reasons for initiating weight-related discussions with ALwO. Additionally, 50% of HCPs reported that unhealthy lifestyle was a factor they considered when deciding whether to initiate weight-related discussions with ALwO.
ALwO who had discussed weight with an HCP reported a mixture of positive and negative feelings after their most recent discussion; 29% of ALwO felt supported and 25% felt motivated, although a similar proportion felt ashamed (29%) and depressed (23%) (online supplemental figure 5). Caregivers who had discussed their child’s weight with an HCP tended to have more positive feelings after the last discussion, with hopeful (47%), supported (44%) and motivated (41%) among the most common feelings described. Fifteen percent of ALwO and 11% of caregivers felt surprised after their most recent weight-related discussion (online supplemental figure 5). Relative to caregivers, a greater proportion of ALwO felt ashamed (29% vs 14%) and a lower proportion felt supported (29% vs 44%) and motivated (25% vs 41%). Among the ALwO and caregivers who had discussed their/their child’s weight with an HCP, 49% of ALwO and 68% of caregivers trusted the HCP’s weight-management advice, and 43% of ALwO and 61% of caregivers felt the HCP understood the difficulties of weight loss.
Overall, 46% of the ALwO who had discussed weight felt comfortable talking to an HCP about their weight; a greater proportion (66%) of caregivers who had discussed their ALwO’s weight with an HCP felt comfortable. However, in terms of barriers to discussing weight, 30% of all ALwO and 11% of all caregivers did not feel comfortable bringing up their/their child’s weight with an HCP (figure 3). In addition, 20% of HCPs did not feel comfortable discussing weight with their adolescent patients with obesity (figure 3). Other barriers selected by ALwO and caregivers included the ALwO already knowing how to manage their weight (selected by 25% and 18%, respectively), not seeing the ALwO’s weight as a significant medical issue (selected by 24% and 22%, respectively) and not wanting to discuss weight with either the caregiver or adolescent being in the room for the respective group (selected by 20% of ALwO and 12% of caregivers) (figure 3).

Barriers to discussing weight with HCPs: (A) barriers reported by ALwO and caregivers; (B) barriers reported by HCPs. (A) Data are the proportions of respondents who chose each statement as a reason for not discussing their/their child’s weight with the ALwO’s HCP, among all UK ALwO and UK caregivers. (B) Data are the proportions of respondents who chose each statement as a reason they may not discuss weight with an ALwO patient, among all UK HCPs. ALwO, adolescents living with obesity; HCP, healthcare professional. Figure adapted from Mears et al.18
Most HCPs (82%) felt they had a responsibility to actively contribute to their adolescent patients’ weight-loss efforts and 76% of HCPs felt motivated to help with these efforts. HCPs often regarded appointment times not being long enough (46%) and having more important health issues to discuss (36%) as barriers to initiating weight-loss discussions with ALwO (figure 3).
Discussion
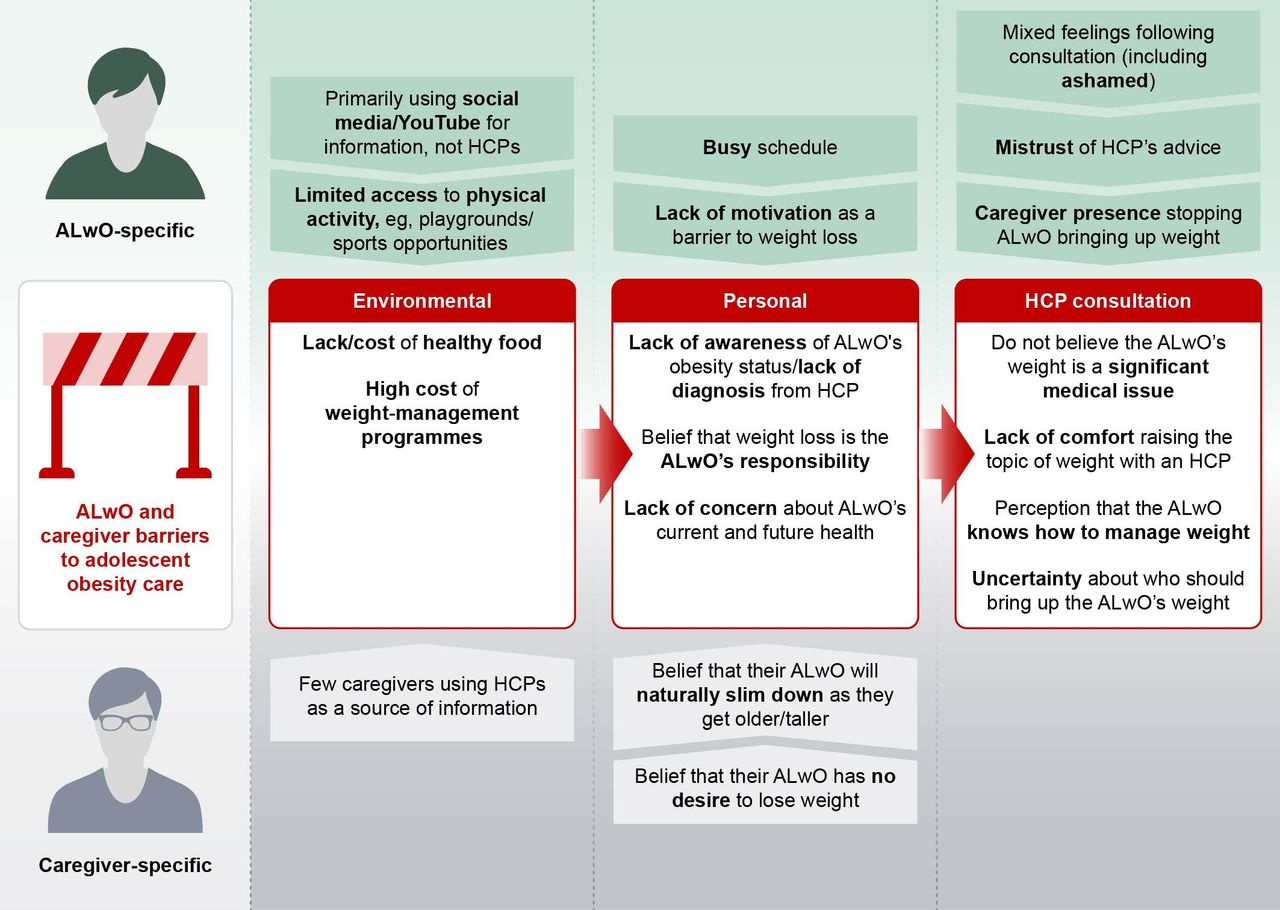
The results from the UK analysis of the ACTION Teens study suggest that there is misalignment among ALwO, caregivers and HCPs and highlight areas where improvements in communication and education are required to enhance obesity care for ALwO in the UK. A summary of the barriers identified for ALwO and caregivers is shown in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of key barriers to adolescent obesity management identified for ALwO and caregivers in the ACTION Teens UK study. Barriers have been grouped into three overarching themes: environmental, personal and HCP consultation-based barriers. Barriers in the middle section (red boxes) apply to both ALwO and caregivers. ALwO, adolescents living with obesity; HCP, healthcare professional.
A large proportion of adolescents did not recognise they are living with overweight or obesity, despite nearly one third of ALwO having class III obesity. In turn, few ALwO were very or extremely worried about their weight and few worried a lot about the consequences of their weight on their future health. There was also a high proportion of caregivers in this analysis with overweight or obesity. In areas of high obesity prevalence, people’s perception of ‘normal’ weight can shift, leading to a distorted perception of their body.26 Additionally, only a small proportion of ALwO and caregivers (10% and 8%, respectively) had been informed by a doctor that they or their child were living with obesity, far fewer than that reported in the global ACTION Teens Study (44% and 29%, respectively).21 This may be due to challenges identifying overweight/obesity because of lack of contact with young people in primary care,27 which may, in turn, have contributed to the underestimation of weight in this analysis.
Most ALwO believed weight loss is solely their responsibility, indicating signs of self-blame and internalised weight stigma. Apparent attitudes of caregivers could partly drive these beliefs; many caregivers believed it would be easy for their ALwO to keep weight off after losing it, and only approximately half of caregivers disagreed that weight loss was entirely their child’s responsibility. Additionally, most HCPs agreed that unhealthy eating habits and lack of exercise are barriers to their ALwO losing weight, and only half of HCPs disagreed that weight loss is entirely the ALwO’s responsibility. These attitudes feed the misconception that weight is a personal choice, and although weight stigma was not directly assessed in our study, these views may be linked to weight stigma and biased attitudes towards ALwO. Obesity should be recognised as a complex, relapsing, long-term condition with multiple causes, including genetics, behavioural and social determinants of health.28 29 Of note, attitudes among HCPs may impact the level of care provided to people with obesity.30 Increasing education on the causes of obesity and ensuring interactions with patients are positive may help to reduce weight stigma among HCPs—such training is needed for those working with ALwO.31
Of interest, our analysis found that approximately half of ALwO and two-thirds of caregivers who had discussed weight with an HCP reported trusting the HCP’s weight-management advice. However, ALwO reported mixed feelings following weight-related discussions with an HCP; 48% reported negative feelings, including ashamed, depressed and blamed, and 30% did not feel comfortable bringing up weight with their HCP. Such negative feelings may be due to experiences and/or internalisation of weight stigma, which is pervasive and can arise from multiple sources, including peers, educators, caregivers, media and HCPs.32 Continued negative experiences and conversations can contribute to depression, anxiety and low self-esteem, and may reinforce feelings of personal responsibility.33 Taken together, these findings highlight the complexity and sensitivity of these interactions, and suggest a need to improve ALwO’s interactions with HCPs. This is also despite policy recommendations and consensus statements outlining the importance of respectful communication about weight, including the use of non-stigmatising language, following evidence of weight bias in healthcare.29 34 A recent review exploring perspectives of young people who access support for mental health found that they need a trusting relationship to discuss sensitive issues—they wanted their HCP to listen to their concerns with empathy and make them feel comfortable.35 Continuity of care, unhurried consultations and a long-term patient–doctor rapport all contributed towards a positive relationship.35
We found that ALwO primarily used social media and YouTube for information about weight. A small proportion of ALwO had sourced information about weight from a doctor, and among those who had discussed weight with an HCP, less than half trusted the advice from HCPs, suggesting an urgent need for HCPs to review communication and engagement strategies for adolescents. A greater understanding of the type and impact of weight-management content that ALwO are viewing on social media could help improve engagement. ALwO may believe accessing information from an HCP is more difficult than via social media due to perceived barriers such as appointment times and few HCPs initiating weight-related discussions. The rapid availability and diversity of information from social media may also be appealing to young people.36 Of note, reliance on online/digital health technologies increased rapidly during the COVID-19 pandemic.37 38 To better communicate with ALwO about weight-management interventions, HCPs should consider a more proactive approach that utilises digital communications and technology.
Although HCPs in this analysis generally recognised they have an obligation to help ALwO manage weight, the presence of obesity-related comorbidities was the most frequently selected reason for initiating weight-loss discussions. Few HCPs (18%) believed they were responsible for initiating these conversations; the majority believed responsibility varies depending on the patient, which calls for further research into who they believe is responsible. Delaying these weight-related conversations and any potential intervention that the ALwO requires may hinder the ALwO’s health in the long term by putting them at greater risk of developing obesity-related comorbidities.12 39 Additionally, short appointment times were identified by HCPs as the main barrier to initiating weight-related conversations with ALwO. The time available for consultations in primary care (on average 9.2 min) is generally limited by a lack of capacity and competing priorities, such as administrative burdens.40 A meta–analysis found that insufficient appointment times were an organisational barrier to HCPs having weight-related discussions with the caregivers of adolescents.41 Furthermore, HCPs felt they had few contact opportunities due to limited routine contact appointments and potential long gaps.41 Difficulties accessing primary care consultations can make it challenging for adolescents to build a relationship with their primary care practitioner.42 43 Professional stakeholders in a UK adolescent weight-management programme echoed that longer-term support was needed for ALwO, although they recognise the current restraints on resources.44 There is a need to address appointment time constraints, the lack of available resources, the importance of adequate training among HCPs, and promotion of healthy lifestyles among ALwO and caregivers when considering future interventions within the UK.
This study has many strengths, including the involvement of three respondent groups (ALwO, their caregivers and HCPs involved in obesity management/treatment) and the stratified sampling and weighting of caregivers’ data to mitigate selection bias. Limitations include the cross-sectional study design, limiting the ability to determine cause and effect; the relatively small sample size; the reliance on self-reported data (height and weight) to determine eligibility, which could have led to an inaccurate BMI and does not provide data on body composition; few ALwO and caregivers being matched; and the possibility of response bias, such as the potential bias towards digitally active participants due to the online nature of the survey. Furthermore, in the UK, the survey was available in English only, limiting respondents to those who could understand English. Therefore, our findings are likely to be most generalizable to English-speaking, digitally active ALwO, caregivers and HCPs. Future studies could involve adolescents/ALwO in the design of questionnaires/studies, explore adolescents’ lived experience of obesity (including its impact on mental health) in greater depth and investigate ways to improve weight-related communications and information sources.
In conclusion, the rising prevalence of adolescent obesity and data from this study highlight a need to improve education and communication among ALwO, caregivers and HCPs in the UK. It is also important to improve trust in HCPs among ALwO to encourage uptake of health services. Additional training for HCPs could help reduce weight stigma and increase understanding of the complexity of obesity, thus empowering HCPs to initiate potentially challenging weight-related conversations with ALwO and caregivers. Recognition of obesity may also improve perceptions of weight among ALwO and caregivers. A whole-system approach to obesity is needed to improve care, including close collaboration with local authorities.45 On an institutional level, the NHS and health sector should consider establishing additional support and education for ALwO, caregivers and HCPs, to increase recognition of obesity as a chronic disease and to reinforce the importance of appropriate weight-related discussions throughout its workforce. Although resources are stretched, adequate consultation times are required to ensure ALwO receive the care, sensitivity and attention necessary and to allow HCPs to address their concerns and build a trusting relationship with ALwO. Weight-related communication strategies in the future should consider using social media and digital technology to improve ALwO’s access to high-quality and trusted information about weight.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data will be shared with bona fide researchers submitting a research proposal approved by the independent review board. Individual participant data will be shared in data sets in a deidentified and anonymised format. Data will be made available after research completion. Information about data access request proposals can be found at novonordisk-trials.com.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved for the UK by the institutional review board of WCG, Puyallup, Washington, USA (tracking number: 20212733; approval date: 27 July 2021). Informed consent was provided by all participants, including a parent/legal guardian of the ALwO. The study was conducted according to the EphMRA Code of Conduct, the principles of the Declaration of Helsinki and applicable laws/regulations related to management of personal information.
Acknowledgments
We gratefully acknowledge the study participants and all personnel involved. We thank Andrea Stoltz, Nick Henderson, Peg Jaynes, Rebecca Hahn and Lynn Clement of KJT Group, especially, for data collection and analysis. Medical writing support was provided by Abbie Richold, of Apollo, OPEN Health Communications and funded by Novo Nordisk A/G, in accordance with Good Publication Practice (GPP) guidelines (www.ismpp.org/gpp-2022).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @brownadey, @Louisa_Ells
Contributors JCGH contributed to the design of the study. JCGH, ACB, KC, LJE, AG, DG, CH and SS participated in interpretation of the ACTION Teens UK data, participated in drafting and revising the manuscript and approved the final submitted version. JCGH is the guarantor for this work.
Funding This work was supported by Novo Nordisk A/G. The study sponsor was involved in study design, analysis and interpretation of the data and funded medical writing assistance and the open access fee for the present manuscript.
Competing interests JCGH reports consultancy fees from Novo Nordisk for his role as a member of the ACTION Teens Steering Committee during the conduct of the study, consultancy fees from Boehringer Ingelheim and Dupont (paid to the University of Leeds), honoraria from Novo Nordisk (paid to the University of Leeds), support from Novo Nordisk for attending meetings and financial support from Dupont for participation in an advisory board (paid to the University of Leeds). ACB reports honoraria from Johnson and Johnson, Novo Nordisk, Obesity UK and the Office for Health Improvement and Disparities, outside the submitted work; he is also on the Medical Advisory Board of, and a shareholder of, Reset Health Clinics. KC reports speaker fees from Apollo Endosurgery and Ethicon, and participation in advisory boards for Boehringer Ingelheim and Eli Lilly; he is also the Chair of Trustees for the patient charity WLSinfo and for the European Coalition for People living with Obesity. LJE receives funding from the Medical Research Council and National Institute for Health and Care Research and is a member of the Office for Health Improvement and Disparities National Child Measurement Programme board and the NHS Complications from Excess Weight Clinics E-board. AG is a full-time employee of Novo Nordisk. DG reports honoraria, speaker fees and support for meeting attendance from Novo Nordisk. CH reports consultancy fees from Ethicon and Novo Nordisk. SS reports honoraria from Merck, Novo Nordisk, Pfizer and Sandoz.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.