Article Text

Abstract
Objective Intellectual disability liaison nurses in general hospitals could enhance access to high-quality, adapted healthcare and improve outcomes. We aimed to explore associations between the input of intellectual disability liaison nurses and the quality of care in people with intellectual disability who are admitted to hospital.
Design Retrospective analysis of a national dataset of mortality reviews.
Setting General hospitals in England.
Participants 4742 adults with intellectual disability who died in hospital between 2016 and 2021 and whose deaths were reviewed as part of the Learning from Lives and Deaths mortality review programme.
Outcome measures We used logistic regression to compare the sociodemographic and clinical characteristics of those who did, and did not, receive input from an intellectual disability liaison nurse. We explored associations between liaison nurse input, care processes and overall quality of care.
Results One-third of people with intellectual disability who died in hospital in England between 2016 and 2021 had input from an intellectual disability liaison nurse. Intellectual disability liaison nurse input was not evenly distributed across England and was more common in those who died of cancer. Having an intellectual disability liaison nurse involved in an individual’s care was associated with increased likelihood of reasonable adjustments being made to care (adjusted OR (aOR) 1.95, 95% CI 1.63 to 2.32) and of best practice being identified (aOR 1.37, 95% CI 1.17 to 1.60) but was not associated with a rating of overall quality of care received (aOR 0.94, 95% CI 0.78 to 1.12).
Conclusions Intellectual disability liaison nurses see only a minority of people with intellectual disability who are admitted to hospital in England. Increasing the availability of intellectual disability liaison nurses could improve care for this disadvantaged group.
- quality in health care
- health policy
- hospitals
- nursing care
- patient-centered care
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study used a large dataset of detailed reviews of care that people with intellectual disability received across England over a period of 5 years.
The study used data only from those who died in hospital.
The level and type of input of intellectual disability liaison nurses were not known in individual cases.
Patient and carer outcome measures were not recorded.
Background
Intellectual disability, also known as learning disability in the UK, is a lifelong disorder of diverse aetiology characterised by significantly below-average intellectual functioning and adaptive behaviour.1 The prevalence of intellectual disability is approximately 1%, with more males than females being affected.2 People with intellectual disability have higher rates of physical illnesses and complex multimorbidity than those in the general population, including neurological disorders, sensory impairments, osteoporosis, metabolic and cardiovascular diseases.3 4 Evidence from across the globe shows that people with intellectual disability are more likely to die premature deaths than their counterparts without intellectual disability, with many of these being potentially avoidable with the provision of good quality healthcare.5–8 Improving care for people with an intellectual disability and reducing health inequalities experienced by this group is a priority for governments and healthcare systems.9
Adults with intellectual disability are more likely than those without to be admitted to hospital and their admissions are longer,10 11 yet they frequently report poor experiences of hospital care.12–14 General hospitals may be ill equipped to meet the needs of people with intellectual disability owing to deficits in staff knowledge and skills,14–16 stigmatising attitudes among professionals17 and institutional discrimination, which together can lead to worse outcomes and avoidable deaths.18
The introduction of intellectual disability liaison nurses (also known as learning disability liaison nurses) has been proposed as one of a range of interventions to improve care experiences and outcomes in hospitals.19 The remit of the intellectual disability liaison nurse is wide-ranging and a tripartite role has been described that includes clinical, educational (training) and strategic (organisational) elements.20 Despite anecdotal evidence of increasing numbers of intellectual disability liaison nurse posts in UK hospitals over the past two decades, no substantive figures exist about their coverage and there has been relatively little systematic or generalisable evaluation of their impact on care.21 The aim of this study was to explore the involvement of intellectual disability liaison nurses in a large cohort of adults with intellectual disability accessing in-patient care in general hospitals and the association of their input with selected care processes and quality of care.
Methods
Data source
Data were obtained from Learning from Lives and Deaths (LeDeR), a national mortality review programme for people with intellectual disability in England. LeDeR was established in 2015 with the aim of improving the quality of healthcare for people with intellectual disability and reducing premature mortality by undertaking comprehensive and independent reviews of the care that deceased people received and identifying areas of both good and poor practice that can inform targeted improvement actions at local or national scale. The development and implementation of the LeDeR programme have been described in detail elsewhere.22
Anyone with an intellectual disability who dies at the age of 4 years or older is eligible for a LeDeR review. Deaths are first notified via a central system; the notifier, who may be a health or social care professional, or a friend or relative of the person who has died, provides key information about the person that enables the LeDeR administrative team to confirm that the deceased individual falls within the scope of the programme (ie, had a confirmed intellectual disability, was ≥4 years at time of death, were registered with a general practitioner in England, and had not opted out of their information being used). The person’s demographic information is then shared with local healthcare commissioners in the region where the person lived, and a trained local reviewer is allocated. The reviewer is an experienced professional with a health or social care background who had not been directly involved in the care of the person who died.
An initial review is completed for each death; this includes a narrative summary of the person who died, information about their health and care needs, and the cause and circumstances of the person’s death, including healthcare interventions received. Multiple sources of information are used to complete the review, including information from discussions with family members or friends of the person who had died, professionals, and primary and secondary care medical records. The reviewer assigns an overall rating to the quality of care that the person received based on a global review of the case, as well as highlighting any learning points (deficits) and areas of good practice that should be shared more widely. The initial review is submitted to the local LeDeR lead professional for a quality assurance check (which may include revision to meet quality standards) before being uploaded to the national system. At this stage, personally identifiable data are redacted to remove names, contact details and places, before being made available to a defined set of researchers under strict data sharing and security protocols. The benefits of using existing data in this population include access to a relatively large cohort that would not be possible if collecting new data and the ability to observe changes over time.
Data used in the present analysis were obtained from the initial reviews of adults (≥18 years) who died in hospital between 1 July 2016 (the beginning of the national LeDeR programme) and the end of 2021 (the last date for which review data were available).
Covariates
We extracted basic sociodemographic data (age at death; ethnicity; usual living situation; geographic region, as defined by general practice registration23) and clinical information (degree of intellectual disability (categorised as mild, moderate, severe and profound); long-term conditions (including physical and mental health problems)) from completed initial reviews. The underlying cause of death was obtained from the Medical Certificate of Cause of Death,24 a standard form completed by a registered medical practitioner who was involved in the person’s care and categorised according to the chapter of the International Classification of Disease, 10th edition.1
Several questions in the LeDeR review require reviewers to identify services and professional input provided to the person within the last 6 months of their life, including whether an ‘acute intellectual disability liaison nurse’ was involved. This is differentiated from ‘community intellectual disability nurse’ and ‘other specialist nurse’ involvement. Community intellectual disability nurses in England are most often based in specialist community teams for people with intellectual disability and could be expected to have only a very limited role when someone is admitted to an acute hospital, for example, providing handover information about a person’s medical and support needs. ‘Other specialist nurses’, in this context, are likely to include nurses with additional training enabling them to extend their scope of practice in a specific field (eg, palliative care nurses, stroke specialist nurses).
We retrieved data on selected care processes and the overall quality of care rating assigned by reviewers. The provision of reasonable adjustments to care and whether best practice was identified was included as a binary ‘yes/no’ variable completed by reviewers; these questions require reviewer judgement, informed by their professional experience and specific training to complete reviews. The nature of any reasonable adjustments or best practice is not explicitly linked to these questions and is likely to be very diverse owing to the heterogeneity of the group and their health conditions and additional needs. Overall quality of care was recorded by reviewers on an ordinal scale between 1 (‘excellent care’) and 6 (‘care fell far short of expected good practice, and this contributed to the cause of death’) (online supplemental table 1).
Supplemental material
Analysis
Data were summarised using descriptive statistics. We created a new multimorbidity variable for those with five or more long-term health conditions. The quality of care rating was categorised as a binary variable; those receiving a grade of 5 or 6 were combined into a new category of ‘poor’ (where the care contributed or had the potential to contribute to, the cause of death) and those with a grading of 1–4 (inclusive) were judged as ‘acceptable/good’ care (where the care received did not contribute to the cause of death).
We used logistic regression to compare the characteristics of those who received input from an intellectual disability liaison nurse with those who did not receive input from an intellectual disability liaison nurse. We calculated unadjusted and adjusted ORs (aOR; adjusting for sex, ethnicity, age at death, degree of intellectual disability, region, marital status, living situation, presence of multimorbidity and cause of death). We then used logistic regression (again adjusted for sex, ethnicity, age at death, degree of intellectual disability, region, marital status, living situation, presence of multimorbidity and cause of death), with intellectual disability liaison nurse input as a predictor variable to test whether their input was associated with markers of quality of care including whether a do not attempt cardiopulmonary resuscitation (DNACPR) order was correctly followed, whether reasonable adjustments to care were made, if best practice was identified as part of the review and overall quality of care rating. We used Wald tests of association and for categorical predictor variables with more than two levels, we reported joint tests. Results were considered statistically significant if p<0.05.
Patient and public involvement
The LeDeR programme includes input from people with intellectual disability as part of the Staying Alive and Well co-production group. The group reviews the findings of the programme, provides a lived experience perspective and is involved in dissemination activities, including creating accessible versions of reports.
Results
Descriptive data
The total dataset comprised 4742 reviews of people with an intellectual disability who died in hospital between 2016 and 2021 (table 1 and online supplemental table S1 with cause of death data). The median age at death was 62 years (IQR 51–71 years). Of the total, 2783 (59%) were male and 4227 (89%) were white.
Demographic and clinical variables of the sample by ID liaison nurse input
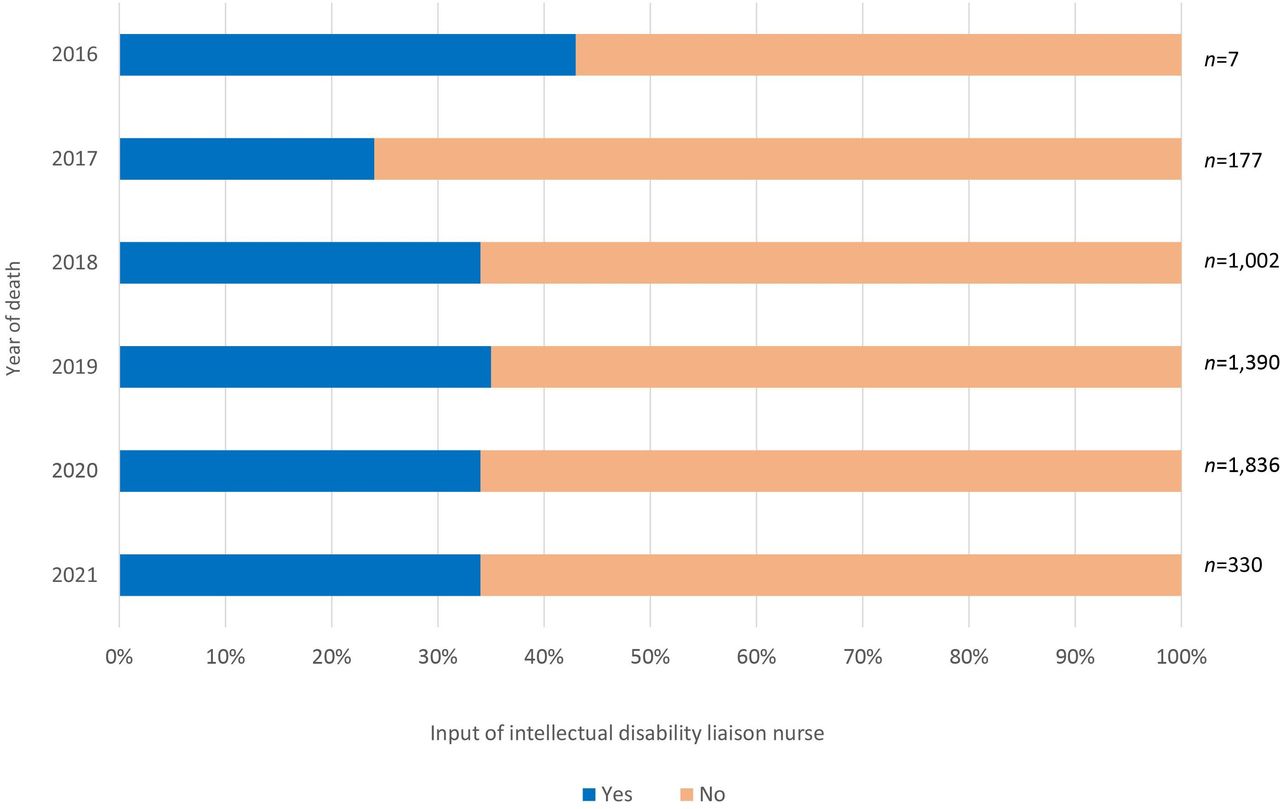
1615 (34.1%) reviews indicated that an intellectual disability liaison nurse was involved in the person’s care in the 6 months prior to their death; this proportion was consistent over the 5 years that data were available (figure 1). Although there was some variation in those who died in 2015 and 2016, interpretation of this is limited by the much smaller numbers of reviews completed in those years.

{kind=link}
Intellectual disability liaison nurse input by year of death (n=4742).
Association of sociodemographic and clinical factors with intellectual disability liaison nurse input
There were statistically significant associations between region, cause of death and the presence of multimorbidity and recorded input from an intellectual disability liaison nurse (table 1). We did not find statistically significant associations between age, sex, ethnicity, level of intellectual disability, and marital status and involvement of a liaison nurse. People living in the North-East of England and Yorkshire and those in the North-West of England were less likely to have received input from an intellectual disability liaison nurse, using the Midlands region as the reference category (aOR 0.74, 95% CI 0.58 to 0.95 and aOR 0.39, 95% CI 0.30 to 0.51, respectively). People who died of cancer were more likely to have had input from an intellectual disability liaison nurse, with the infectious diseases category as the reference (aOR 1.98, 95% CI 1.09 to 3.61). People with multimorbidity, defined as five or more long-term health conditions, were more likely to have input from an intellectual disability liaison nurse (aOR 1.37, 95% CI 1.14 to 1.66). Those who lived in supported community living or a residential home were more likely than people living in their own homes to be seen by an intellectual disability liaison nurse, though these results fell marginally outside statistical significance.
Association of intellectual disability liaison nurse input with care processes and quality of care
Involvement of an intellectual disability liaison nurse was significantly associated with reasonable adjustments being made to care (aOR 1.95, 95% CI 1.63 to 2.32) and best practice being identified by the reviewer (aOR 1.37, 95% CI 1.17 to 1.60) (table 2 and online supplemental table S2 with unadjusted ORs). Intellectual disability liaison nurse input was not significantly associated with grading of overall quality of care (aOR 0.94, 95% CI 0.78 to 1.12).
Supplemental material
Association of ID liaison nurse input with care processes and quality of care rating
People who received input from an intellectual disability liaison nurse were more likely to have a DNACPR order in place at the time of their death (aOR 1.41, 95% CI 1.18 to 1.69), however, input from a liaison nurse was not associated with the likelihood of the DNACPR order being correctly completed or followed (aOR 0.81, 95% CI 0.55 to 1.17).
Discussion
Summary of key findings
Specialist intellectual disability liaison nurses have been recommended to work across general hospital departments to improve the experience and outcomes of people with intellectual disability who are admitted to hospital. Our data show that only a minority of adults with intellectual disability who died in hospital in England between 2016 and 2021 received input from an intellectual disability liaison nurse prior to their death. This may be due to a person’s intellectual disability not being recognised or recorded when they are admitted to hospital meaning that they are not identified as being eligible for specialist input.25 Alternatively, it may be that not all hospitals employ intellectual disability liaison nurses or, where they do, coverage is limited by resource constraints or because the post is split across a number of sites. It is not mandatory for hospitals in England to employ an intellectual disability liaison nurse service and no national-level data exist that show the extent of intellectual disability liaison nurse provision in hospitals. A survey of children’s hospitals in England found that just over half had a dedicated intellectual disability nurse.26 A recent NHS benchmarking exercise found that 30% of staff in NHS secondary care services did not have access to specialist intellectual disability advice, although respondents included those working in community and mental healthcare settings, as well as those in hospitals.27
The regression analysis showed certain patient-level characteristics were significantly associated with the likelihood of receiving input from an intellectual disability liaison nurse. After adjusting for other factors, people who died in the two regions covering the north of England were significantly less likely to have seen an intellectual disability liaison nurse prior to their death. This may be due to difficulties in recruitment or retention of specialist staff in those areas. Intellectual disability nurses represent only a small proportion of all nurses in the UK and their numbers are falling.28
Cancer is the fourth most common cause of death in people with an intellectual disability29 and those who died of the condition were most likely to receive input from an intellectual disability liaison nurse. This might be because of relatively well-resourced and structured care pathways for people diagnosed with cancer and their integration with palliative care services for people with a terminal diagnosis that has a holistic and multidisciplinary focus. It is also possible that those with cancer tend to be admitted to larger hospitals which may be more likely to have intellectual disability liaison nurse input.
People with multiple long-term health conditions were more likely to receive input from an intellectual disability liaison nurse. It may be that the input of an intellectual disability liaison nurse was sought by the responsible care team in these cases due to the complexity of care being increased, or it may also be that intellectual disability liaison nurses prioritise these cases where their resource is limited. Although not statistically significant, we also observed that people living in supported or residential care were more likely than those living in their own home to receive the support of a specialist nurse; this may be because paid carers advocated for greater input in the hospital. It might also be due to intellectual disability not being recognised in people with less significant functional impairments (who live independently), although there was no observed association between degree of intellectual disability and liaison nurse input.
DNACPR orders provide guidance to medical staff about how to respond when someone has a cardiac arrest.30 DNACPR decisions are not legally binding and are not signed by the patient or a witness (in contrast to Advance Decisions to Refuse Care) but should be discussed with the person and their family or carers, where possible. Previous research has shown considerable variation in how DNACPR policies are written and enacted for the general population, with significant scope for improvement.31 32 In addition, there has been renewed focus on the appropriateness and rigour of the DNACPR process since the COVID-19 pandemic, with people with intellectual disability considered at particular risk of poor and discriminatory practice, including blanket policies to deny CPR based on a diagnosis of intellectual disability or specific genetic conditions.33 The finding that the involvement of an intellectual disability liaison nurse was associated with an increased likelihood of a DNACPR order being made perhaps suggests that the nurse can facilitate necessary end-of-life care discussions, including about DNACPR and avoiding inappropriate and futile resuscitation attempts. However, liaison nurse input was not associated with the quality of DNACPR documentation or whether the order was correctly followed; this may indicate that the liaison nurse’s influence is limited in a medically driven process or that they were not closely enough involved in the direct care of the person to provide advice and oversight about implementation when a decision has been made.
Under the UK Equality Act,34 hospitals and other providers of services have a legal duty to make reasonable adjustments to ensure that people are not disadvantaged by nature of any protected characteristic, including disability. In the context of intellectual disability, reasonable adjustments to hospital care may include environmental adaptations on the ward, providing information in accessible formats, or permitting carers to remain with a person outside usual visiting hours.35 A core component of the intellectual disability liaison nurse’s role is to ensure person-centred care when someone is admitted to hospital36; this was clearly evident in the findings which showed that those with input from a liaison nurse were almost twice as likely to receive any reasonable adjustments to care. Similarly, there was more likely to be evidence of best practice in the person’s care when their case was reviewed where an intellectual disability liaison nurse was involved. Best practice here is broadly defined and could include good practice when dealing with families and carers, following guidelines, or applying the principles of the Mental Capacity Act.37 One previous audit of hospital in-patient care of people with intellectual disability in England found that there were improvements in markers of high-quality care (including having appropriate assessments and care plans in place) in those hospitals where an intellectual disability liaison nurse was employed, but this study was underpowered and could not directly link care of individual patients to liaison nurse input.38
In contrast, there was no observed association between input of an intellectual disability liaison nurse and overall quality of care rating assigned by the reviewer. This question requires the reviewer to consider all aspects of care that the person received, not limited to healthcare or care received in hospital and includes a multitude of factors that an intellectual disability liaison nurse could not reasonably be expected to have any influence over, such as quality of support provided in the person’s home or the appropriateness of community activities. Nonetheless, our findings seem to indicate that the input of an intellectual disability liaison nurse is associated with tangible benefits for the individual. Qualitative studies that have included people with intellectual disability and carers have reported that intellectual disability liaison nurses are highly valued20 and improve hospital experiences for people with intellectual disability, including in communication, patient safety, holistic care and the provision of reasonable adjustments.15 36 39
Strengths and limitations
There is little existing evidence of the impact of intellectual disability liaison nurses on objectively measured patient-level care outcomes. To our knowledge, the intellectual disability liaison nurse role has not been implemented beyond the UK and the Ireland,21 despite international evidence of poor care provision for this group.38
We obtained data from a very large national dataset of in-depth individual reviews of the care that people with intellectual disability received before their death. Reviews are completed using a standardised method by trained reviewers who can access a person’s complete medical record and who gather data from a range of sources, including by speaking to informants who knew the deceased person in either a personal or professional capacity. The reviews are of deaths that occur across all regions of England over a period of 5 years and findings can be considered representative on this basis. There are very low rates of missing data in each variable and the data gathered can be trusted as accurate and comprehensive. We were able to identify factors associated with the likelihood of receiving input from an intellectual disability liaison nurse, potentially highlighting disparities in access to care. The study adds to the limited empirical evidence of the impact of intellectual disability liaison nurses on individual outcomes which, given the largely positive findings, could be used to strengthen existing recommendations for acute hospitals to provide this service.
Although reporting deaths to the LeDeR programme is strongly encouraged, it is not mandatory and there may be a small number of people who died who are eligible for a LeDeR review who did not receive one; we do not have their details and are not able to characterise this group. The dataset includes only those people who have died, and therefore we are not able to draw inferences about the input and impact of intellectual disability liaison nurses for people who are admitted and later discharged from the hospital.
This study is a secondary analysis of data that were collected to improve services but not specifically to answer our research questions, and our analysis is limited by the data that are available. Intellectual disability liaison nurse input was identified using a single yes/no question, which cannot identify variation in the type or degree of involvement in individual cases. Liaison nurse models of working may differ between hospitals and across the country, but we do not have information available to define liaison models in use and to associate these with outcomes. As this is an observational study, we are not able to determine the direction of associations that were shown between intellectual disability liaison nurse input and other variables. We have no clear measure of patient or carer experience or reported outcomes and how these may have been influenced by input of an intellectual disability liaison nurse. Although there are safeguards to ensure LeDeR reviews are standardised, there may have been some unmeasured variability in how individual reviewers classified good practice or rated quality of care.
Further work
A national census of intellectual disability liaison nurse posts would provide more detailed information about coverage and access to specialist care and identify where gaps exist. This would also help to define different modes of liaison nurse work at organisational and individual levels which could be evaluated in a prospective study to determine the optimum model of liaison working. A health economic evaluation as part of this would demonstrate the financial implications of the role and is important where there are competing demands on the healthcare budget. It will be important that future work extends the current study by including people who did not die in hospital; this could be achieved through sampling those who have been identified as having intellectual disability on their discharge documentation or by using linked datasets. This could also include people who attend the hospital as outpatients as well as those who are admitted. It would also be possible to expand the evaluation to new settings, to examine the benefits of intellectual disability liaison nurses in primary care or acute mental health services.
The perspectives and experiences of people with intellectual disability and family carers should be sought so that practice advances can take these into account. Such studies may be conducted as in-depth qualitative evaluations, appropriately adapted to enable the participation of people with communication needs, and would complement the potential national-scale work described above.
Conclusion
The addition of intellectual disability liaison nurses to acute hospitals has been proposed as a means of improving the effectiveness and safety of care for people with intellectual disability and their hospital experience. Intellectual disability liaison nurses have a broad remit spanning direct involvement in individual cases, providing support and training to healthcare staff, taking a strategic role in interpreting national policy and embedding a positive organisational culture around intellectual disability care. The role is not universal in hospitals in England and there may be regional variations in access to liaison nurse care. Our work lends support to the value of intellectual disability liaison nurses in general hospitals but further research is needed to determine the most clinically effective and cost-effective models of care and to determine the impact on patient and family carer experience.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The LeDeR programme uses data from human participants who are deceased. The programme has Section 251 approval from the Health Research Authority’s Confidentiality Advisory Group, on behalf of the Secretary of State, which permits the processing of identifiable data without consent. Specific additional ethical approval was not needed for this study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @dr_rorysheehan, @drandrestrydom
Contributors RS, JD, AW, NM, UC, KM-T and AS contributed to study conception, planning and design. RS, AW, JD and NM extracted and analysed study data. RS, JD, AW, NM, UC, KM-T and AS interpreted the data. RS was responsible for drafting the manuscript and for revisions. RS, JD, AW, NM, UC, KM-T and AS reviewed the final manuscript and approved the decision to publish. RS acts as guarantor.
Funding The LeDeR programme is funded by NHS England. An academic collaboration, led by King’s College London, is commissioned to analyse LeDeR data.
Disclaimer No specific funding was received for this work and the funders had no role in analysis, review, or approval of the manuscript, or decision to submit the manuscript for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.