Article Text

Abstract
Introduction HIV is a major global public health issue. The risk of sexual transmission of HIV in serodiscordant couples when the partner living with HIV maintains a suppressed viral load of <200 copies of HIV copies/mL has been found in systematic reviews to be negligible. A recent systematic review reported a similar risk of transmission for viral load<1000 copies/mL, but quantitative transmission risk estimates were not provided. Precise estimates of the risk of sexual transmission at sustained viral load levels between 200 copies/mL and 1000 copies/mL remain a significant gap in the literature.
Methods and analysis A systematic search of various electronic databases for the articles written in English or French will be conducted from January 2000 to October 2023, including MEDLINE, Embase, the Cochrane Central Register of Controlled Trials via Ovid and Scopus. The first step of a two-step meta-analysis will consist of a systematic review along with a meta-analysis, and the second step will use individual participant data for meta-analysis. Our primary outcome is the risk of sexual HIV transmission in serodiscordant couples where the partner living with HIV is on antiretroviral therapy. Our secondary outcome is the dose-response association between different levels of viral load and the risk of sexual HIV transmission. We will ascertain the risk of bias using the Risk Of Bias in Non-randomised Studies of Interventions (ROBINS-I) and Quality in Prognostic Studies (QUIPS), the risk of publication bias using forest plots and Egger’s test and heterogeneity using I2. A random effects model will estimate the pooled incidence of sexual HIV transmission, and multivariate logistic regression will be used to assess the viral load dose-response relationships. The Grading of Recommendations, Assessment, Development and Evaluation system will determine the certainty of evidence.
Ethics and dissemination The meta-analysis will be conducted using deidentified data. No human subjects will be involved in the research. Findings will be disseminated through peer-reviewed publications, presentations and conferences.
PROSPERO registration number CRD42023476946.
- HIV and AIDS
- Sexually Transmitted Disease
- Public health
- Systematic Review
- Epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THE STUDY
The proposed individual participant data (IPD) meta-analysis will be conducted using raw data from individual participants with advantages, including greater quantity of data, more flexibility in analytic approaches, the ability to conduct subgroup analyses and improved ability to detect and address biases.
This innovative two-step meta-analysis will still collect and synthesise evidence and answer the research questions even if the IPD part is not feasible.
Studies collected in the review may have differences in the timing and frequency of viral load testing, adherence to antiretroviral therapy and patient follow-up, causing imprecision within the data.
There may be insufficient data across the full range of viral load levels to fully assess the association and/or potential lack of agreement by authors to share data for the IPD meta-analysis.
Introduction
Globally, an estimated 39 million people are currently living with HIV (PLHIV), of whom 29.8 million (76%) are on treatment and 21.2 million (54% of all PLHIV and 71% of PLHIV on treatment) are living with suppressed HIV.1 Antiretroviral therapy (ART) can improve the lives of PLHIV and help protect their sexual partners from sexual HIV transmission. People who are on HIV treatment can achieve an undetectable viral load with effectively no risk of transmitting HIV to their sexual partners.2 This concept is referred to as Undetectable equals Untransmittable, or U=U,3 and it was initiated in 2016 by the Prevention Access Campaign, a health equity initiative with the goal of ending the HIV/AIDS pandemic and associated HIV-related stigma.4 The U=U concept is based on a substantial body of scientific evidence demonstrating that for PLHIV who have achieved a sustained suppressed and undetectable viral load, there is effectively no risk of sexual HIV transmission.5 Furthermore, treatment as prevention is one of the effective strategies to prevent HIV transmission, with high uptake of ART suggested as an effective approach to reduce HIV incidence.6 7
A systematic review and meta-analysis published by the Public Health Agency of Canada (PHAC) in 2018, concluded, using criteria defined by the Canadian AIDS Society framework to characterise HIV transmission risk,8 that the risk of sexual transmission of HIV is negligible when the PLHIV is on ART with a suppressed viral load of <200 copies of HIV RNA/ml with consecutive testing every 4–6 months.2 A rapid review published by the Canadian Agency for Drugs and Technologies in Health (CADTH) in 2023 as well as a 2023 PHAC rapid communication confirmed these findings, with the PHAC report providing an estimated risk of HIV sexual transmission of 0.00 transmissions per 100 person-years (95% CI 0.00 to 0.10) in this specific situation.9 10 In 2023, a systematic review by Broyles et al11 concluded that the risk of sexual transmission of HIV is almost zero when the PLHIV is under ART and has a suppressed viral load of <1000 copies of HIV RNA,11 but no quantitative risk estimate was calculated. Furthermore, the WHO concluded in its 2023 policy brief that PLHIV who have a suppressed but detectable viral load have almost zero or negligible risk of sexual transmission of HIV to their partner as long as they continue to take their ART as prescribed.12 The WHO also revised the operational definition for undetected viral load from ‘≤ 50 copies/ml’ to ‘not detected by the test or sample type used’ and suppressed viral load from ‘≤200 copies/ml’ to ‘≤1000 copies/ml’ and recommended a viral suppression threshold of 1000 copies/mL because persistent viral load levels above 1000 copies/mL are associated with treatment failure.12
Most of the literature demonstrating that a suppressed, undetectable viral load is associated with effectively no risk of sexual HIV transmission uses a viral load threshold of 200 copies/mL.3 5 Precise estimates of the risk of sexual transmission at sustained viral load levels between 200 and 1000 copies/mL remain a significant gap in the literature. Addressing this gap by quantifying these risks is needed to evaluate the strength of the association between different viral load levels and the risk of HIV transmission, and to better understand considerations of viral load levels with respect to HIV treatment and prevention programmes.
The primary objective of this review is to quantify the risk estimate of HIV transmission and determine the association between different levels of viral load (primarily in the range 200–1000 copies/mL) and the risk of sexual HIV transmission among serodiscordant couples where the PLHIV is on ART.
The specific hypotheses include: (a) there will be a significant difference in the risk of sexual HIV transmission between viral load levels and (b) there will be a dose-response relationship between different viral load levels (200 copies/mL, 400 copies/mL, 1000 copies/mL or >1000 copies/mL) and risk of sexual HIV transmission.
Research questions
Q1: What is the risk of sexual transmission of HIV with suppressed viral load<1000 copies/ml and at different levels of viral load>1000 copies/ml?
Q1.1: What is the risk of sexual HIV transmission in serodiscordant couples when the PLHIV is on ART with different levels of suppressed viral load between 200 to 1000 copies/ml (new potential evidence on risk of HIV transmission with viral load<200 copies/ml will also be assessed and reported if available)?
Q1.2: What is the risk of sexual HIV transmission in serodiscordant couples when the PLHIV is on ART with different levels of viral load>1000?
Q2: Is there a dose-response association between different levels of viral load and the risk of sexual HIV transmission?
Methods and analysis
Patient and public involvement
In designing this meta-analysis protocol, neither patients nor public were involved.
Protocol guidance and registration
This systematic review will follow a two-step meta-analysis approach. First, a systematic review and meta-analysis will be conducted. Second, an individual participant data (IPD) meta-analysis will be performed if feasible. IPD is considered as the gold standard of reviews and has several advantages compared with aggregate data systematic reviews and meta-analyses. These advantages include a greater quantity of data, the ability to standardise outcomes across trials, more flexibility in analytic approaches, the ability to conduct subgroup/moderator analyses and an enhanced ability to detect and address biases.13 This protocol is based on the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocol (PRISMA-P) statement14 (online supplemental appendix table 1). This systematic review and meta-analysis will follow the methodology outlined in the Cochrane Handbook for Systematic Reviews of Intervention.15 16 The reporting of results will follow the PRISMA 2020 and PRISMA-IPD meta-analysis guidelines (online supplemental appendix tables 1,2).17 18 IPD meta-analysis will be done using data from studies already published or ongoing on this topic. Although such an approach would produce the best theoretical result, there are some limitations with this method,19 namely the potential for insufficient data across the full range of viral load levels and/or potential lack of agreement by authors to share such data. Based on the results of the included studies from full-text screening of studies, we will be selecting collaborators for IPD requests. If the proposed IPD meta-analysis is not possible, the systematic review will assess the extent to which these research questions can be answered from existing published literature alone.
Supplemental material
Supplemental material
Protocol registration
This study has been registered with the International Registration of Systematic Reviews (PROSPERO) on 11 November 2023 with the registration number CRD42023476946 . Any future changes or modifications to the review procedures will be documented and updated to the PROSPERO registration.
Eligibility criteria and type of study
Original studies (randomised controlled trials and non-randomised studies), case reports and conference abstracts will be included if they report on longitudinal studies of couples with one partner living with HIV and document the number of HIV infections in previously seronegative sexual partners and provide information about viral load levels in the HIV-seropositive partner and/or use of ART. For studies that report any HIV infections in the seronegative partner, they will need to be linked to the partner living with HIV through phylogenetic analysis to rule out infection from outside the couple. Considering the difficulty of doing individualised randomisation in public health interventions, cluster Randomized Controlled Trials (RCTs) and quasi-experimental studies with self-control will also be considered for inclusion. Studies reporting a sex partner living with HIV who takes ART and has a viral load measurement provided will be included. Articles written in English and French will be retrieved from electronic English and French databases with full-text access, and published within the timeframe of 1 January, 2000 to Oct 2023 will be included.20 Studies involving condom use or pre-exposure prophylaxis will be excluded. Studies where HIV is not primarily transmitted through sex will also be excluded. Reviews, editorials, letters and conference proceedings without detailed results will be excluded. Search types and patterns are featured in online supplemental appendix 2.
Participants, type of interventions and outcomes of interest
Information sources and search strategy
A comprehensive and systematic search of the following databases will be conducted: MEDLINE, Embase, the Cochrane Central Register of Controlled Trials via Ovid and Scopus. The search strategy, developed by a health information professional in collaboration with the other authors, uses text words and relevant indexing to identify studies on viral load, ART and transmission of HIV between serodiscordant couples. The MEDLINE search strategy (see Appendix) will be applied to all databases with appropriate modifications. The search will be limited to publications from January 2000 to 2023.
In addition, a thorough examination will be performed of the reference lists of identified relevant studies, experts in the field of HIV sexual transmission will be contacted to identify any additional studies or results, and ClinicalTrials.gov and International Clinical Trials Registry Platform will be examined to identify planned, ongoing or unpublished trials. To retrieve any grey literature, Google Scholar and Baidu Scholar will also be searched. Clinical trial registries will also be searched, including the US National Institutes of Health’s clinicaltrials.gov and Health Canada’s Clinical Trials Database. Search types and patterns are featured in online supplemental appendix table 3.
Supplemental material
Study selection
Articles will be imported and deduplicated using EndNote20 (Clarivate, Philadelphia, Pennsylvania, USA) and then imported into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) for screening. Reviewers (GB, JD and PVN) will do pilot screening with a sample of 100 abstracts to ensure consistency of use and clarity of the inclusion and exclusion criteria. To measure the inter-rater reliability, a Cohen’s kappa statistic will be used. Screening will begin when >70% agreement is achieved.21 In duplicate, the authors (GB, JD and PVN) will conduct all screening, data extraction and quality assessment procedures. Disagreements will be resolved by consensus. Situations where consensus cannot be reached will be resolved by a third author who will arbitrate (PD and HB). Eligible articles identified by title and abstract screening based on inclusion criteria will be selected for full-text screening. Two independent reviewers will review the full texts. References of the included studies will be hand searched to identify additional relevant studies for inclusion. Conflicts between reviewers will be resolved through discussion, and if no resolution can be achieved, a third reviewer (PD and HB) will be consulted. In case of missing data or information, authors will be contacted.
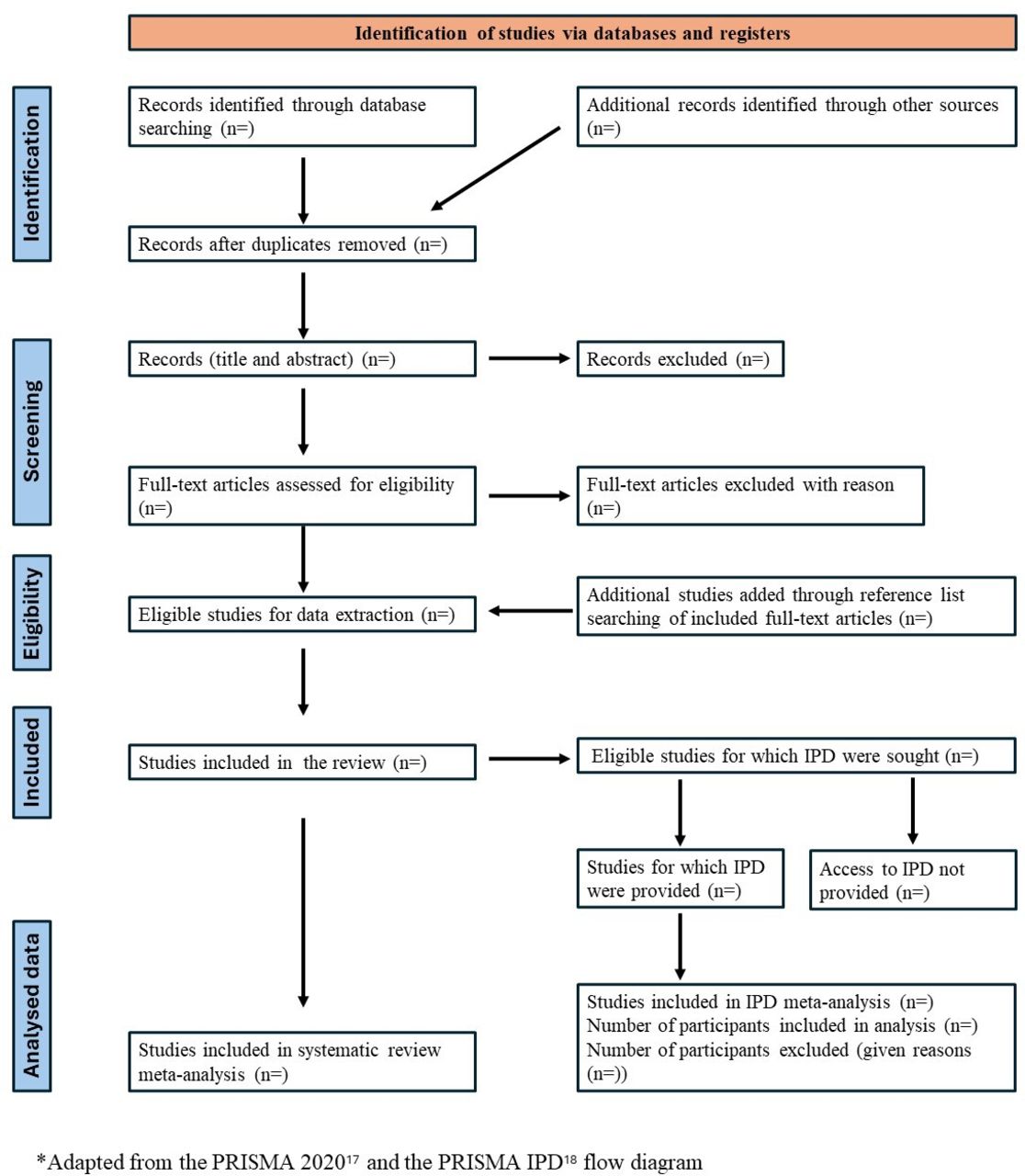
A third reviewer (PD and HB) will confirm the excluded publications and their respective reasons for elimination. A PRISMA flow chart adapted from the PRISMA 2020 and the PRISMA IPD flow diagram (figure 1)17 18 will be used to show the process of study selection.

{kind=link}
PRISMA flow diagram. IPD, individual participant data; PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis.
Data extraction and management
After the full-text screening and study selection process, the selected studies will undergo data extraction, wherein information from the studies will be extracted after a thorough reading of the full text. The list of variables to be extracted is presented in table 1. The data extraction form will be created using Microsoft Excel 2016. Data extraction will be conducted by two independent reviewers using the designed data extraction form. Following this process, the records extracted by the reviewers will be cross-checked, and any disputed points will be resolved through a third reviewer (PD and HB).
List of variables for data extraction.
Risk of bias assessment
For non-RCTs, the ROBINS-I (the Risk Of Bias in Non-randomised Studies of Interventions) tool will be used by the reviewers to determine the quality of the study. The ROBINS-I tool is concerned with evaluating the risk of bias in estimates of the effectiveness or safety (benefit or harm) of an intervention from studies that did not use randomisation to allocate interventions.22 This will influence how the data are interpreted. For prognostic studies, QUIPS tool will be used.23 Biases will be measured as ‘critical risk’, ‘serious risk’, ‘moderate risk’, ‘low risk’ and ‘no information’.
The risk of publication bias will be assessed by visual inspection of funnel plots and using the Egger’s test (with 10 or more included articles).24
Data synthesis
Descriptive statistics from included studies will be extracted and summarised in tables. When there is a difference in data units across studies, we will perform data conversion for the meta-analysis. The main statistical analysis of the study will involve two steps:
Meta-analysis using data extracted from included studies
Incidence data will be summarised for meta-analysis. A pooled estimate of the incidence of sexual HIV transmission will be generated and reported with 95% CI. Heterogeneity will be examined using25 26 the I2 and the H² statistics since they both relate to the percentage of variability that is due to true differences between studies (heterogeneity). I² will be quantified as low (≤25%), moderate (25%–50%) or high (>50%). Fixed-effect model will be used for heterogeneity <50%. Where heterogeneity is >50%, we will use the random-effect model to examine the association between varying viral loads and risk of HIV transmission among serodiscordant couples and create summary forest plots.
The variation for moderate or higher heterogeneity will be explored by conducting meta-regression and sensitivity analyses, including sample size, study year and demographic characteristics, or excluding studies to examine heterogeneity. Furthermore, we will also attempt to explain the heterogeneity by conducting subgroup analyses to compare the risk of HIV transmission between groups, including gay, bisexual and other men-who-have-sex-with-men (gbMSM), women who have sex with women and heterosexuals.
The presence of publication bias will be assessed using a funnel plot and Egger’s test, provided we have at least 10 studies included in the meta-analysis.24
Statistical analysis using IPD
A data sharing agreement will be established outlining the nature of the project, collaboration and responsibilities of each party. Deidentified and anonymised participant data will be confidentially collected from collaborators. Descriptive analyses will be performed to examine the participants’ demographic characteristics.
We will analyse all the studies separately to compare our results with the original study. Any discrepancies will be resolved. Analysis will include all study participants following the intention-to-treat approach. Summary statistics will be presented as mean (SD) or median (IQR) for continuous variables and per cent for categorical variables. Effect size will be computed for different thresholds of viral load. χ2 test will be used to evaluate the association of viral load to the risk of sexual HIV transmission by comparing the various viral load levels. We will also compute ORs and corresponding 95% CI to assess the strength of the association of viral load to the risk of sexual HIV transmission. The level of statistical significance α will be 0.05 for all tests. An individual random-effect meta-analysis will be conducted to determine the overall effect of viral load on sexual HIV transmission. Furthermore, a multivariable logistic regression for binary outcomes will be done to predict the risk of HIV transmission among serodiscordant couples at different levels of viral load at the baseline level from each study. Additional adjustments with sociodemographic characteristics, including age, sex, education and location, will also be included. Effect sizes and standard errors can be obtained from this analysis including covariate adjustment which could potentially address bias concerns.
Additionally, viral load levels will be categorised into a contingency table to investigate whether different viral load categories are associated with different levels of HIV transmission risk among sexual partners. A dose-response relationship will also be examined between different viral load levels in PLHIV and the incidence of HIV among their partners using multivariate logistic regression and incidence frequencies of sexual HIV transmission.
All analyses will be done in R V.4.2.3, REVMAN and SPSS V.28 as needed.
Missing data
Missing data will be addressed depending on the specific characteristics of the missing data. An effort will be made to discuss with collaborating teams the possibility of collecting missing data from their studies. If the data are missing completely at random for the entire study, a list-wise or pair-wise deletion to obtain valid and complete cases will be performed. However, this step may reduce the sample and power of the study. For the remaining non-random missing data, multiple imputations by chained equations will be used.27 In this method, missing data is computed on a case-by-case basis. A regression model will also be conditionally applied to the other variables in the dataset.
Certainty of evidence
Summary of findings will be presented via tables, including tables for each of the prespecified outcomes (eg, number of cases of HIV transmission). The Grading of Recommendations, Assessment, Development and Evaluation will be used to assess the certainty of evidence considering the bias risk of the trials, consistency of effect, imprecision, indirectness, publication bias, dose response and residual confounding.28
Ethics and dissemination
The meta-analysis will be conducted using deidentified and anonymised data. No human subjects will be directly involved in this research. Dissemination of results of this review will be done through peer-reviewed publications and presentations, as well as international conferences.
Discussion
We understand that effort, resources and international cooperation are required to perform meta-analysis based on IPD. We will produce a meta-analysis based on the number of collaborators interested in this review and the quality of data collected. We will attempt to establish quantitative risk estimates of sexual HIV transmission at viral load levels between 200 copies/mL and 1000 copies/mL and potentially also at levels >1000 copies/mL. This two-step systematic review (SR) and individual participant data (IPD) meta-analysis will also evaluate the strength of the association of viral load to the risk of sexual HIV transmission. The findings of this SR and IPD meta-analysis will help patients, researchers and policymakers to better understand the risk of sexual HIV transmission in the context of ART and the associated considerations for HIV treatment and prevention programmes.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors PD, HB, CA and AF participated in the conception and design of the study. PD, HB, CA, and TE developed the search strategy and assessed the feasibility of the study. PD, HB, GB, JD and PVN wrote the manuscript. CA improved the manuscript. PD, HB, CA and AF are the guarantors. All the authors critically reviewed this manuscript and approved the final version.
Funding This research was funded, conducted and approved by the Public Health Agency of Canada.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.