Article Text

Abstract
Introduction The growing population of older drivers presents challenges for road safety attributed to age-related declines and increased crash fatality rates. However, enabling older people to maintain their health and independence through continued safe driving is important. This study focuses on the urgent need for cost-effective interventions that reduce crash risk while supporting older drivers to remain driving safely for longer. Our study aims to evaluate the effectiveness of three behavioural interventions for older driver safety. These include an online road-rules refresher workshop, tailored feedback on driving performance and two tailored driving lessons.
Methods and analysis A single-blind three-parallel group superiority randomised controlled trial will be conducted with 198 urban licensed drivers aged 65 years and older, allowing for 4% attrition. This sample size provides 80% power to detect a difference with an alpha of 0.05. Participants will be selected based on a standardised on-road test that identifies them as moderately unsafe drivers. Interventions, spanning a 3-month period, aim to improve driving safety. Their effectiveness will be assessed through a standardised on-road assessment of driving safety at 3 months (T1) and 12 months postintervention (T2). Additionally, monthly self-reported driving diaries will provide data on crashes and incidents.
This trial has the potential to identify cost-effective approaches for improving safety for older drivers and contribute to evidence-based health policy, clinical practice and guidelines.
Ethics and dissemination Ethical approval was obtained by the University of New South Wales Human Research Ethics Committee (HC190439, 22 August 2019). The results of the study will be disseminated in peer-reviewed journals and research conferences.
Trial registration number ACTRN12622001515785.
- Ageing
- Risk management
- Randomized Controlled Trial
- PREVENTIVE MEDICINE
- Aged
- Cognition
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
To our knowledge, the largest randomised control trial assessing tailored driver training interventions over a 12-month period in older drivers.
Process evaluation and cost-effective analysis included to provide practical recommendations to road users and authorities.
Larger sample size would allow for greater generalisability of results.
Introduction
Background
An ageing population is resulting in an increasing number of older drivers on the road. In Australia, approximately 92% of adults aged 70+ are licensed drivers and expect to keep driving well into their 80s.1 Driving enables social engagement and independent living;2 however, driver crash rate, consequent fatality and healthcare costs are a concern.3 Reports indicate drivers aged 65 years and older have crash fatality rates equivalent to those of drivers aged 17–25.4 Consequently, improving on road safety of older drivers is an important public health challenge.
The normal ageing process results in a reduction of driving skills,5 6 and is associated with increases in crash rates4 and increased fatality risk.7 The normal ageing process includes declines in visual, sensorimotor and cognitive capacities, which are associated with physiological and brain ageing,6 8–10 suboptimal driving skills10–13 and lack of awareness of the change regarding driving abilities;11 14 all of which have been identified as predictors of unsafe driving.
After involvement in on-road crashes, older drivers may restrict their driving or cease driving altogether,15 16 even if they are medically fit to drive. Studies indicate that driving enables social participation which reduces loneliness and social isolation.16 17 Maintaining the safety of older drivers on the road for as long as possible promotes healthy ageing, independence and longevity.18 As a result, driver remediation strategies should be considered for at-risk older drivers before cessation of driving.19
Targeted training of older drivers may be a viable remediation strategy, but currently, there are limited training options available to improve road safety and reduce crash rate for at-risk older drivers who are medically fit to drive. Some driving schools offer courses for older drivers; however, there is no regulation regarding the content of these courses or evidence regarding whether they are effective. Currently, very few interventions have been evaluated using a randomised controlled trial (RCT) design and predictors of intervention effectiveness have rarely been explored.20 As a result, there is a paucity of information on which components of driver training are essential to be effective for older drivers.
Heterogeneity in the components of older driving training programmes trialled previously, and outcomes used to measure their effectiveness add to this problem. Prior research has shown that classroom education programmes improve older drivers’ knowledge21 but when evaluated independently do not lead to improvements in driving skill and safety.21–23 When assessing driver training methods, many studies combine on-road training with classroom education;21 24–27 however, there may be a distinction between the two, with on-road training shown to improve safety to a greater extent than classroom education alone.24 26 28 Previous studies also frequently combine on-road training with feedback on driver performance, with some interventions using standardised driving lessons with verbal feedback21 24 25 and others incorporating tailored videos of on-road errors into the feedback content.24 26 28 Using on-road safety scoring systems, independent from the driver training received and with assessors blind to group allocation, the aforementioned studies found that on-road driver training was associated with improved driver safety.
In a pilot study, we assessed the feasibility and effectiveness of driver trainer interventions as a means of improving older driver safety.24 In a sample of 57 older drivers aged 65 years and older (mean age 72.0, 47.4% male), the effectiveness of tailored driving lessons combined with feedback was compared with the effectiveness of a road rules refresher course. Using the Driver Safety Rating (DSR) score based on an on-road assessment of the total number and severity of driver errors, our study found that common driving errors were reduced by 20%–30% compared with baseline, which is consistent with previous findings.22 26 28
Three studies of those described above, evaluated video feedback of drivers’ performances,22 24 26 but only one evaluated video feedback independent of other interventions.22 This study (n=54) found that video feedback was associated with a 25% reduction in errors on the on-road test (ORT) when compared with classroom education or no-contact controls at 4 to 6-week follow-up. To identify the effectiveness of the individual components of the intervention, further work with larger sample sizes is required. In addition, while these studies have consistently shown the benefits of interventions to reduce driver errors and improve on-road performance, the longevity of these effects is not clear due to short follow-up periods (up to 3 months). Furthermore, there has been little attention to behaviour change principles in the design or description of intervention components incorporated in older driver training interventions. This is a common problem in public health interventions29 which have not clearly incorporated behaviour change principles into trial designs, and predictors of intervention effectiveness have not yet been explored.
Aims and objectives
The primary aim of this study is to evaluate the effectiveness of interventions to improve older driver safety in a superiority RCT. Participants will be randomly assigned to one of three training programs, with some components provided online. These include (1) a Road Rules Refresher workshop, (2) tailored Feedback with action planning plus the workshop or (3) two tailored Driving Lessons plus Feedback and the workshop. Intervention effectiveness will be assessed independently of interventions by measuring driving performance in an ORT undertaken at three time points: baseline, 3 months (primary outcome) and 12 months (secondary outcome 1). We hypothesise that the Driving Lesson-Plus-Feedback intervention will be more effective than the Feedback intervention, and both will be more effective than the Road Rules Refresher intervention, in improving drivers’ safety rating over 3 months and 12 months.
Additional secondary objectives include evaluating the effect of the interventions on (1) critical driving errors; (2) health-related quality of life over 12 months; (3) driving self-efficacy; (4) social participation; (5) incremental cost-effectiveness ratio for the improvement in driver safety and (6) number of self-reported crashes and near misses over a 12-month period. The study will also evaluate whether individual characteristics such as performance on baseline laboratory-based driving safety screening measures and cognitive tests predict outcomes within the intervention groups.
Materials and methods
Study design
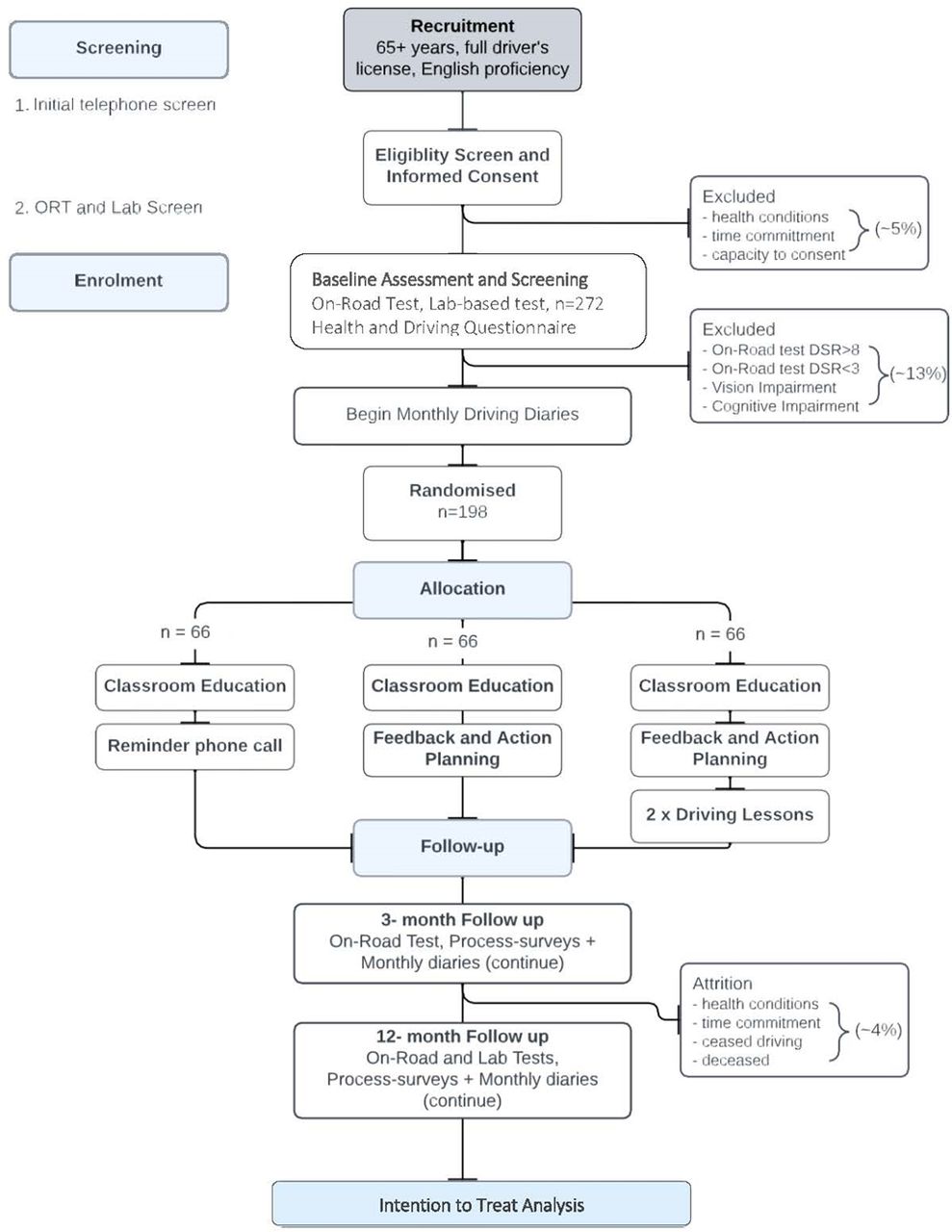
This study is a three-arm, single-blind superiority RCT. The three arms will comprise the following conditions: Control: Road Rules Refresher Workshop (C); Intervention I: Feedback (F) plus C; Intervention II: Driving Lessons-Plus-Feedback (L+F) plus C. Follow-up assessments will occur at 3 months (T1) and 12 months (T2) postintervention. The interventions involve a tailored approach, using a lesson prescription from the baseline ORT and applying individual remediation strategies through feedback and/or lessons. The Road Rules Refresher Workshop is prerecorded and is standard for all participants. This study will evaluate the superiority of the interventions (F and L+F) against the active control group (C) receiving driver education training only. The trial design and study process are illustrated in figure 1. Allocation will follow a 1:1:1 ratio and participants in all groups will be evaluated at three time points: baseline, 3 months and 12 months. All participants will provide electronic or written consent to participate in the study (online supplemental appendix A). This protocol was written in accordance with the Standard Protocol Items: Recommendations for Interventions Trials checklist.30
Supplemental material

{kind=link}
Trial design and study processes. ORT, on-road test.
Study setting
The study will be conducted at a single site in a community setting with fully licensed drivers drawn from the suburban population in Sydney, Australia. Participants will be community-dwelling individuals aged 65 years and older. A rolling recruitment strategy seeks to enrol 198 participants via print advertising, web-based and social media, community and consumer groups, sporting clubs, volunteer sites and primary care providers. No financial incentives will be provided for participation.
Eligibility criteria
Eligibility will be assessed in three stages: telephone eligibility screening, baseline lab assessment, and baseline on-road assessment before selection into the trial. Trial inclusion criteria include age >65 years, current license, insurance, English skills and baseline on-road safety rating in the moderate range. Trial exclusion criteria include recent driver refresher training, low visual acuity, cognitive impairment and serious mental or physical health conditions that may affect participation. These criteria will be assessed as described below.
Screening and enrolment process
Screening and enrolment will be implemented by trained researchers. First, participants will provide verbal consent to answer a series of eligibility questions over the telephone. These questions will ascertain whether participants are of age ≥65 years, have a current driver’s licence with minimum third-party car insurance in the Sydney metropolitan area, have sufficient English language skills to complete written questionnaires and follow instructions, absence of significant mental or physical health conditions that would prevent full participation in the study or impaired driving ability (eg, cognitive impairment, major stroke, current cancer treatment, antipsychotic medication, narcotic pain medication, significant visual field loss and uncorrected visual impairment) or experience with older driver refresher courses within the last 5 years. Second, participants will attend a 90-min lab-based assessment during which a battery of sensory and cognitive tests will be administered by a trained research assistant. Participants with a visual acuity score below 6/12 binocularly (minimum requirement for driver licensing in Australia) will be asked to self-refer to an optometrist before being reconsidered for study inclusion. Participants scoring 23 or below on the Montreal Cognitive Assessment (MoCA31) will be screened as having significant cognitive impairment sufficient to impact participation in the study. This cut-off has a sensitivity of 83% and specificity of 94% in identifying mild cognitive impairment.32 Participants with low scores are recommended to see their General Practitioner for follow-up.
Participants meeting the above criteria will undertake a baseline ORT following a standardised urban route in traffic (see description in outcome measures). The ORT will be conducted in a dual-brake vehicle with a driving instructor (Assessment-DI) seated in the passenger seat and assessed by a driver-trained occupational therapist (Assessment-OT; accredited with the Australian Health Practitioner Regulation Agency) seated in the backseat, both of whom will be masked to the participants’ laboratory-assessment results. The ORT will follow a standardised assessment protocol used in our previous studies24 which provides a 10-point DSR scale ranging from 1 (high risk/very unsafe driver) to 10 (low risk/very safe driver). Drivers will be identified as having low on-road safety risk and excluded from trial enrolment if they score at or above 8/10, suggestive of limited opportunity to improve behaviours based on our previous pilot trial. Drivers will be identified as having high on-road safety risk and excluded from trial enrolment if they score at or below 3/10. It is recommended to participants in this category that they consult their general practitioner and may be counselled by a driver-trained occupational therapist to seek further clinical investigation of their driving safety. The DSR cut-off has been validated in prior studies and estimated to comprise 5% of community-dwelling older drivers.24 Drivers who meet all inclusion criteria and no exclusion criteria will be enrolled in RCT.
Randomisation and blinding
Participants will be randomised to either Control: Road Rules Refresher Workshop (C); Intervention I: Feedback (F) plus C or Intervention II: Driving Lessons-Plus-Feedback (L+F) plus C following a 1:1:1 ratio across the three groups (66 per group). Allocation will be stratified by age group (65–74 years; 75+ years), given age-related changes in cognitive and sensorimotor abilities and sex due to known gender differences in driving; this is consistent with our previous trial.24 The study statistician will use stratified blocked randomisation with a randomly selected block size (3/6/9) to generate the randomisation sequence. Allocation will be automated with participant assignment to conditions based on the concealed randomisation sequence implemented through a Research Electronic Data Capture (REDCap) database.
The randomisation sequence and assignment will be concealed from all researchers, including the research assistants conducting lab-based tests, the Assessment-DI and Assessment-OT. During the follow-up assessments, participants will be reminded not to discuss their group allocation with the assessment team, and the Assessment-OT will wear noise-cancelling headphones during the on-road assessment to prevent inadvertent disclosure of allocation by participants. Those not blind to allocation include the trial manager responsible for enrolling, obtaining consent, scheduling participants and monitoring study progress, the Intervention-DI and Intervention-OT responsible for the driving lessons and feedback, respectively, and the participants themselves. All other investigators including chief investigators, statistician, Assessment-OTs, Assessment-DIs and those conducting the laboratory assessments will be blind to group allocation during the trial.
Interventions
Interventions will be implemented by driver-trained OTs and qualified DIs, referred to as the Intervention-OT and Intervention-DI, respectively. The intervention team consists of one OT and four DIs who are independent of the assessment team.
Control arm: Road Rules Refresher Workshop
Participants in the control arm will complete an online, prerecorded 1 hour Road Rules Refresher Workshop and receive a copy of the 2022 New South Wales (NSW) Road Users Handbook. The Road Rules Refresher Workshop will be prerecorded by an independent Intervention-DI and attendance monitored by the trial manager. The Workshop will educate older drivers on the effects of ageing on driving ability, the NSW state requirements for licensing checks for older adults, examples of common errors that older drivers make and how to remediate these errors and will provide a refresher on relevant road rules. Participants will receive a phone call during week 2 to remind them of the workshop for the purpose of controlling for any potential social interaction benefits experienced in the face-to-face components of Intervention I and II.
Intervention I: Feedback
Participants in the Feedback condition will receive the Road Rules Refresher Workshop and a 1-hour online tailored feedback session with the Intervention-OT. Using the lesson prescription from the baseline ORT,24 the Intervention-OT will discuss the participant’s driving performance, focusing on the three driving weaknesses identified based on the frequency and severity of driving errors. Using motivational interviewing and goal-directed behaviour modification techniques,33 targeted driving errors will be discussed for remediation, outlining the importance of safe driving practice and identifying strategies to remediate the driving error. Video clips from the participant’s baseline ORT will be used to demonstrate the errors made. At the end of the feedback session, participants will receive a homework booklet including their action plan comprising a summary of goals tailored to the participant for correcting errors or habits in a standard format. This will be sent fortnightly for 12 weeks, providing reminders and rehearsal of intervention goals, and recording of self-ratings on progress. The homework sheets are sent and received via REDCap.
Intervention II: Driving Lessons-Plus-Feedback
Participants in the Driving Lessons-Plus-Feedback condition will receive Intervention I plus two driving lessons. Driving lessons will be conducted by the Intervention-DI where the participant will receive guided on-road training and review of specific skills. Skills for remediation are identified in the baseline ORT Lesson Prescription. The prescription focuses on both errors identified during ORT as well as areas that need remediation, identified by the Assessment-OT. Lesson 1 will be conducted in a dual-brake vehicle and include on-road driving practice using routes within or near the participant’s usual driving environment. Lesson 2 will be conducted in the participant’s own vehicle and include routes within or near the participant’s usual driving environment, with further application of those refreshed skills in unfamiliar areas. As lesson 2 will be conducted in the participant’s own vehicle, the participant will be asked to provide a copy of their current third-party car insurance prior to the lessons. Lessons will be approximately 7 days apart. Intervention-DIs will be asked to submit a lesson summary at the end of each lesson outlining the driver skills covered in the lesson. These will be compared with the skills identified in the lesson prescription to ensure intervention consistency.
Adherence
The Road Rules Refresher Workshop will be completed in the participant’s own time with completion submitted via REDCap. Adherence is monitored by the trial manager who follows up with participants who have not indicated they have completed the workshop. Trial participants in Intervention I and II will receive fortnightly homework sheets that monitor their adherence to the goals set in the feedback session. Participants will be asked to report whether or not they have implemented any of the safe driving skills and rate how well they think they are doing. If participants have not practised their safe driving skills, they will be asked about obstacles preventing practice to help identify barriers to remediation. At T1 and T2, participants will be asked to complete a process survey which will collect data on adherence, relevance, enjoyment and satisfaction.
Concomitant training
Participants will be asked to refrain from taking any driver education, training or remediation throughout the course of their study involvement. They will be asked about concomitant training in the process survey at T1 and T2. If throughout the course of study participation, it is identified that a participant has received alternate driver training, they will be withdrawn from the study.
Outcomes
Primary outcomes
DSR score
Primary outcome data is collected from the ORT at baseline 3 months (T1) and 12 months (T2) after the delivery of the interventions. The primary outcome is the mean change in DSR score from baseline to T1. The DSR score is derived from the objective ORT conducted by the Assessment-OT and Assessment-DI. Participants will take part in an on-road driving test, 12.3 km in length and approximately 30–35 min, in a dual-brake vehicle. The Assessment-DI directs the participant along a standardised set route in Eastern Sydney suburbia, in off-peak traffic conditions during 10:00 am–02:00 pm. The same route is used at baseline T1 and T2. The standardised route is designed to assess participants’ ability to negotiate a range of common intersections (eg, traffic-light controlled intersections, roundabouts, give-way signs and stop signs), hazards (eg, pedestrian crossings, speed control chicanes and school zones), manoeuvres (eg, lane change, merge, left turn and right turn) and varying road types (eg, dual carriageway, single lane and one-way). Participants will be given time to familiarise themselves with the vehicle and drive around a large parking lot before commencing the test.
About 25% of the driving route will involve self-navigating to the local hospital using road signage, as older drivers typically make proportionally more errors under self-navigation than instructional navigation.34 For each manoeuvre during the test, the Assessment-OT notes errors in observation, head checks, indication, lane positioning, braking, gap selection, speed control and approach. Each error is rated in terms of its severity from 1 to 4, with 1 indicating minor or self-corrected errors and 4 representing errors requiring the Assessment-DI to intervene to avoid a collision. The DSR score is derived from the total number and severity of errors, and the number of critical errors (see below), ranging from 1 to 10 with higher scores indicating greater safety and better driving skills. The DSR score is derived from a scale on which performance is rated and provides a cut-point with scores of 1–3 indicating generally ‘Unsafe/High risk’ driving, 4–7 indicating ‘moderate risk’ and scores of 8–10 indicating ‘low risk/safe’ driving. Our previous research shows the inter-rater reliability of the DSR score, calculated by the OT, to be high (intraclass correlation=0.94 (95% CI 0.93 to 0.95)).24
Secondary outcomes
Secondary outcomes include mean change in the DSR score from baseline to T2, the mean change in number of critical errors recorded during the ORT from baseline to T1 and T2, the number of self-reported traffic incidents reported over the 12-month period and adjusted for mileage, as well as the mean change in health-related quality of life, driving self-efficacy, social participation from baseline to T2 and cost-effectiveness.
Self-reported traffic incidents
Self-reported traffic incidents will be collected monthly through an online driving diary from the time of enrolment to study completion. Subjective estimates of the number of kilometres driven by the participant in the previous month, any crashes, or any significant incidents (ie, near-misses) with a brief description of the event are recorded. Participants are encouraged to track the odometer reading for the measure of kilometres driven per month. In the case of a crash or significant incident, the trial manager will call the participant and collect detailed notes on the incident. Self-reported traffic incidents obtained from monthly injury diaries have been shown to be associated with the ORT both retrospectively and prospectively, such that drivers who commit more errors on the ORT also report more self-reported traffic incidents.35
Critical errors
The number of critical errors made during the ORT is also recorded. Critical errors constitute unsafe manoeuvres that are either (a) ‘dangerous errors’ (requiring DI preventive action) or (b) ‘instant fail driving errors’ that would result in an immediate fail during an on-road licence test (eg, failing to stop at a stop sign). Critical errors are scored by the Assessment-OT during the ORT; the greater the number of critical errors, the less safe the driver is.
Descriptive, health and well-being measures
Participant characteristics will be collected via an online survey, with the option of paper-based, at baseline and T2. The General Health and Driving Questionnaire collects information regarding demographics, health and well-being variables known to impact on or be impacted by driving performance and mobility (table 1). Demographic information collected will include age, gender, education, living arrangements and driving experience, including years of driving experience, kilometres driven over the last 12 months, frequency of long-distance driving and driving space. Health and well-being collected will include alcohol consumption, history of falls over the last 12 months, balance and mobility,36 medical conditions and medications, exercise and activity,37 quality of life (EQ-5D-5L38), social participation (SPQ39), driver self-efficacy (Adelaide Driving Self-Efficacy Scale, ADSES40), mood and cognitive activity engagement. Changes in quality of life, social participation and driver self-efficacy will be measured from baseline to T2.
Summary of outcomes measured by data collection points.
Cost-effectiveness of interventions
A within-trial cost-effectiveness analysis and cost-utility analysis will be conducted to determine whether the two interventions represent ‘value for money’ compared with current practice over the 12- month period. Intervention costs will be determined from the project financial records, including staff time associated with data collection, driving lessons and off-road feedback. Costs associated with self-reported crashes will use 2016 National Roads and Motorists' Association (NRMA) estimates.41
Additional measures of functional performance relevant to driving
Off-road driver screening measures
Off-road driver screening measures of cognitive ability, visual function and mobility will be used to help predict the on-road driver performance.6 The measures below are used to screen and monitor the impact of age-related declines at baseline and T2, as undertaken in our previous studies.6
Cognitive performance
Cognitive function will be measured by the MoCA31, which contains 30 items assessing short-term memory, visuospatial abilities, executive functions, attention, concentration, working memory, language and orientation to time and place. The MoCA has 89% sensitivity and 90% specificity in detecting mild cognitive impairment with a score of 23 or less.32 Additional measures of executive function (trail making test A and B42 and symbol digit modality test43), perceptual-motor abilities (Benton visual retention test44), verbal learning and memory (Hopkin’s verbal learning test revised45) and decision-making (game of dice test46) will be collected.
Visual function
Visual function will be assessed using two tests undertaken binocularly. Static high-contrast visual acuity will be measured using the Australian vision chart 5, which uses logMAR principles, at a working distance of 4.0 m (National Vision Research Institute, Melbourne). Letter contrast sensitivity will be determined using the Pelli-Robson chart under the recommended testing conditions. Visual function will be assessed with the participant’s habitual driving glasses for each individual eye and then both. Participants will be required to receive a logMAR score of 0.30 or better (6/12) with both eyes on the static high-contrast visual acuity test to be eligible for study participation.
Off-road driver safety screening tests
Four off-road driver safety screening tests that have been reported to screen for unsafe driving or crashes in older adults form part of the laboratory assessments. These include1 the useful field of view subtest 2, a computer-based test of visual processing speed and divided attention with high reliability and validity shown in other large studies to predict crash risk;47 ,48 ,2 the occupational therapy—driver off road assessment test,49 a pen-and-paper maze test for which time taken to complete the maze has been associated with driving performance, similar to other maze tests;27 ,50 ,3 the Multi-D, a computer-based test that includes three subtests—choice colour reaction time (requiring hand and foot responses and inhibition of responses), a test of sensitivity to central visual motion (using random dot stimuli presented at 3.2 m), and a test of balance or postural sway (using a sway metre to measure body displacement at the level of the waist)—and has been associated with on-road safety ratings;9 51 and4 DriveSafe/DriveAware,52 a computer-based commercially available clinical screening tool for driving safety.53 The DriveSafe component of this test will be used, which requires participants to view each of the 15 images of the same roundabout intersection for 3 s, then verbally report details about the position and direction of travel of pedestrians and vehicles in the image.52
Data management
There are three data collection points: baseline, 3-month follow-up (T1) and 12-month follow-up (T2). Not all assessments will be conducted at each time point (table 1). Data collection will take place in person or via REDCap, a secure data management system hosted by University of New South Wales (UNSW).54 55 All study and administrative data will be treated with strict confidentiality—collected, managed and stored according to the terms of our ethical approval. Personal information will be stored on secure servers at Neuroscience Research Australia for a minimum of 15 years, in accordance with the UNSW Data Management Policy and Australian data protection regulations. Research data will be deidentified using ID numbers and only accessible to researchers involved in the study.
Data monitoring
The trial will be monitored by the study investigators. The primary investigator will meet the research team weekly to review the study progress, including recruitment, randomisation and assessment completion. The trial has been approved by the Human Research Ethics Committee at the UNSW, Australia.
Quality assurance and fidelity
All researchers involved in the data collection, eligibility assessments and intervention implementation will be trained via a structured training protocol, specific to their study involvement. The Assessment-DI and Assessment-OT will go through rigorous training by senior personnel, combining theoretical content with practice activities, including practice drives. Assessment ORTs are privy to regular checks of reliability (between the DI, OT and independent-rater) and intervention fidelity (content included in the lesson prescriptions) with a random selection of one in every 10 ORTs per assessor. Where possible, 10% of drives will be co-rated by an independent driver-trained OT sitting in the vehicle. Additional video recordings may be evaluated. Fidelity to the intervention protocols will be assessed in a random selection of 10% of the sessions by senior personnel, stratified by interventionist and intervention session.
Sample retention
The trial manager will contact participants to book assessments and complete COVID-19 safety screening checks prior to onsite attendance. Scheduled study-related reminders for assessments will be sent out to participants through email with a follow-up call if required. Online assessments required to be submitted at different time intervals will be sent automatically to the participant through the REDCap survey system, with a maximum of two automated reminder emails per assessment.
Adverse event reporting
For this study, an adverse event will be defined as an unwanted and usually harmful outcome (eg, fall, cardiac event and collision). The event may or may not be related to the intervention but occurs while the person is participating in the intervention or study assessments (ie, while they are doing lab assessments, ORT or engaging in the interventions). Any adverse events will be reported to UNSW Human Research Ethics Committee within 72 hours.
Patient and public involvement
Members of the public were not involved in the design of the study protocol, but intervention design, length and content were informed by feedback and process surveys drawn from one published24 and one unpublished pilot study. The current trial will include process evaluation of all interventions. Dissemination of findings (format and content) will be informed by consultation with a consumer panel that includes study participants at the end of the trial.
Sample size
The intended sample size is 198, with 66 participants in each group. Sample size calculation was conducted via a power simulation which indicated that a sample of 198 participants, allowing for the expected rate of attrition, is required to achieve at least 80% power to detect a difference between the three groups at one-time point, if the true difference between feedback and classroom education and between Driving Lessons-Plus-Feedback and Feedback is 0.5 SD
Statistical analysis
The primary outcome of DSR will be analysed in a linear mixed effects model with random intercepts, fixed effects of intervention (included on an intention-to-treat basis) and time and their interaction. All pairwise comparisons between the three intervention groups at T1 (3 months) will be conducted, with the Benjamini-Hochberg procedure used to control the false discovery rate at 5% across comparisons. The same procedure will be used to analyse intervention effectiveness at T2 (12 months), self-report traffic incidents over the 12-month follow-up and the additional secondary outcomes 12 months’ postbaseline. Missing data for analysis of secondary outcomes will be imputed using multiple imputation with chained equations under the assumption of missing at random56). A minimum of 10 datasets will be imputed, and auxiliary variables will be taken from the baseline survey. Exploratory analysis will evaluate the effect of adherence and practice on outcomes.
Process evaluation
The process evaluation for the project will use mixed methods to examine the quality of the intervention, acceptability and sustainability. Data on adherence, relevance and enjoyment will be collected from the intervention workbooks. Process surveys at 3 months and 12 months will be collected and analysed using descriptive statistics and logistic models.
Cost-effectiveness
For the cost-effectiveness analyses, outcomes of interest will be the DSR and self-reported traffic incidents, while the cost-utility analysis will use health-related quality of life, estimated with the EQ-5D-5L. Regression models will be conducted for both costs and outcomes to estimate the incremental cost-effectiveness ratio between interventions, to determine whether the interventions are considered value for money. Sensitivity analyses will determine the robustness of the results through parameter uncertainty.
Discussion
Crashes involving older drivers not only impose a major financial burden, costing Australia over $1 billion per annum, but also have long-term impacts on the quality of life of those injured and their families.4 Despite a lower overall exposure to driving, older adults are at increased risk of crashes4, and ceasing to drive can lead to increased risk of social isolation.16 In light of an ageing population, society needs to develop strategies that enable older adults to maintain both their mobility, independence and driving safety. This study addresses an important evidence gap in older driver road safety, contributing new knowledge on older driver behaviour and potential remediation strategies.
In a world first, the Better Drive Trial aims to evaluate the effectiveness and cost-effectiveness of driver training interventions in healthy older drivers over a 12-month period. Using a high-quality superiority RCT design, the study’s extended follow-up period of 12 months, provides robust evidence on the impact of cost-effective interventions aimed at enhancing driving safety among older drivers. Our study has the potential to make a major contribution to a field where there is a scarcity of research. The practical applications are far-reaching, with the potential to inform public safety measures, shape health policy and refine clinical practice and guidelines for older driver safety.
Trial status
At the time of manuscript submission, this trial is in the follow-up phase. Participant recruitment opened on 3 January 2023; baseline data collection finished September 2023 and follow-up data collection is expected to be completed by September 2024.
Ethics and dissemination
Ethical approval was obtained by the University of New South Wales Human Research Ethics Committee (HC190439, 22 August 2019). This study has been prospectively registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12622001515785). The results of the study will be disseminated in peer-reviewed journals and research conferences. Study participants, including those screened ineligible, will be provided with a summary of results.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Jasmine Price for her contributions to the study and assessor training.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AH coordinated data collection and drafted the manuscript. KJA is the chief investigator, guarantor, obtained funding, planned and designed the study; JW, KK, KD, MB, JB, LC and TL are co-investigators and contributed to obtaining funding and study plan and design. RE contributed to study plan, design and coordination. KK developed statistical plan. All authors critically reviewed, provided intellectual input and final approval of the manuscript.
Funding This work was supported by the National Health and Medical Research Council (grant number APP1156940); KJA is funded by ARC Laureate Fellowship (grant number FL190100011), KD is funded by NHMRC Investigator Grant (APP1193766). The funders had no role in the trial design and will not have any role during its execution, analyses, interpretation of the data or decision to submit results.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.