Article Text

Abstract
Background A number of devices have been developed to minimise operator radiation exposure in the setting of cardiac catheterisation. The effectiveness of these devices has traditionally been explored in transfemoral coronary procedures; however, less is known for the transradial approach. We set out to examine the impact of three different radiation protection devices in a real-world setting.
Methods and design Consecutive coronary diagnostic and intervention procedures are randomised in a 1:1:1 ratio to a shield-only protection (shield group), shield and overlapping 0.5 mm Pb panel curtain (curtain group) or shield, curtain and additional 75×40 cm, 0.5 mm Pb drape placed across the waist of the patient (drape group).
The primary outcome is the difference in relative exposure of the primary operator among groups. Relative exposure is defined as the ratio between operator’s exposure (E in μSv) and patient exposure (dose area product in cGy·cm2).
Ethics and dissemination The protocol complies with good clinical practice and the ethical principles described in the Declaration of Helsinki and is approved by the local ethics committee. The results of the trial will be published as original article(s) in medical journals and/or as presentation at congresses.
Trial registration number NCT03634657
- coronary heart disease
- coronary intervention
- radiation biology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the largest study investigating the effect of two radiation protection systems on radiation exposure for interventional cardiologists using the radial access.
Allocation is performed in a randomised fashion.
Blinding was not possible.
Exposure is measured only at chest level.
Background
Despite improvements in radiation protection achieved in recent years, interventional cardiologists continue to be exposed to low-dose radiation. Radiation exposure is associated with both deterministic damage (the most common ones being cataract for the operator and skin lesions for the patient) and with a stochastic risk for various malignancies, among which left-sided brain tumours are the most worrisome ones.1–6 In a recent meta-analysis, posterior lens opacities were significantly more prevalent in interventional cardiologists (RR=3.2), and the risk increased with increased career length.7 8
Factors such as operators experience, X-ray equipment, procedure type, patient characteristics (in particular body mass index) and arterial access influence the amount of scattered radiation to which operators are exposed,9–11 and the increasing complexity and number of interventions contributes to a further increase in radiation exposure.
A number of devices and strategies have been developed and investigated to address this risk, including radiation caps, disposable gloves and lead-free shields, ceiling-attached aprons, robotic systems, as well as improved X-ray technologies.12–18 Importantly, most of these studies refer to investigations conducted through the femoral access. However, the radial access for coronary angiography and interventions is associated with lower bleeding risk and improved prognosis in both the elective and acute setting,19–21 and most catheterisation laboratories have progressively switched from femoral to radial programmes. While it remains unclear whether the radial access is associated with increased operators' exposure once the learning curve has been completed,9 11 the additional strategies previously developed to mitigate this hazard need to be retested in this modified setting.
Aim of the study
The aim of the study is to compare the efficacy of three combinations of radiation protection devices for the reduction of the relative operators' radiation exposure in the setting of radial coronary procedures. These results may provide recommendation on which (combination of) device(s) provide the best protection in this setting.
Methods and design
This is a prospective, single-centre, randomised and parallel group design trial conducted in the catheterisation laboratory of the Kardiologie I, University Medical Center Mainz, Germany. Consecutive coronary diagnostic and intervention procedures are assigned in a 1:1:1 ratio to one of the three radiation protection groups described below.
The SPIRIT checklist for reporting a clinical trial was used.22 Data acquisition started in August 2018. The duration of this study is expected to be 16 months.
Study setting
The University Medical Center of Mainz is a high-volume tertiary clinic. Experienced cardiologists and fellows (under supervision) perform invasive exams and operate the X-ray equipment.
Study intervention
Investigation medical product
Radiation protection
Procedures will be randomised to one of three groups:
A ceiling-mounted, 60×76 cm, 0.5 mm Pb, shield-only protection (shield group).
Shield and overhanging 0.5 mm Pb panel curtain (curtain group).
Shield, curtain and additional 75×40 cm, 0.5 mm Pb, drape placed across the waist of the patient (drape group).
A scheme of the interventions is presented in figure 1.

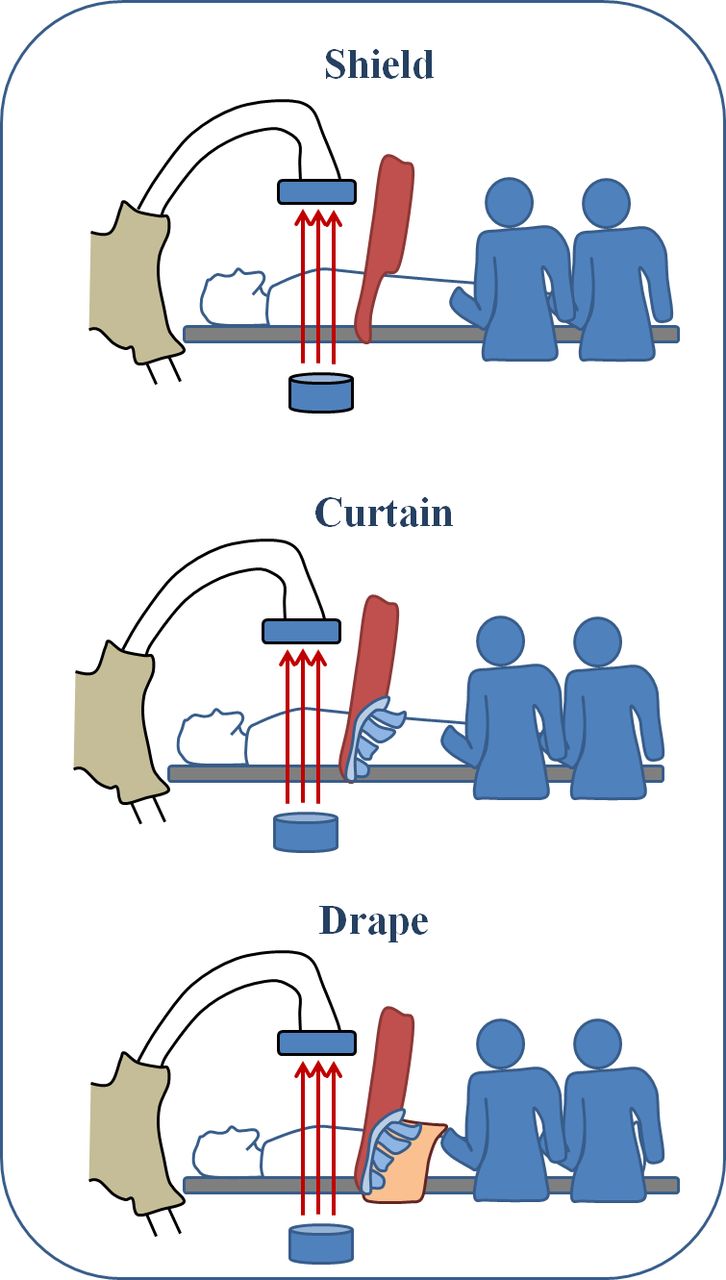{kind=link}
Schematic representation of the three interventions. The shield (red), curtain (blue) and drape (orange) are presented.
Conventional radiation protection measures (lead aprons, lead collar) will be used in all three groups. All procedures will be performed using the same X-ray equipment (Philips AlluraClarity FD10, Philips Medical Systems).
Study objectives
Primary outcome
The primary outcome is the difference in relative exposure of the primary operator among groups. Relative exposure is defined as the ratio between operator’s dosimetry (in μSv) and patient exposure (dose area product in cGy·cm2).
Co-primary endpoint is the difference in relative exposure of the assistant operator among groups
Secondary objectives
Secondary outcomes include:
Difference in patient exposure among groups.
Difference in operators' absolute dose among groups.
Difference in both primary outcomes in subanalyses limited to:
diagnostic versus interventional procedures.
procedures in patients with body mass index (BMI) ≥30 vs<30.
Analysis of predictors of operator and assistant operator exposure including BMI, age, sex, type of procedure (diagnostic versus interventional, biopsy, duration, contrast used, recanalisation, use of additional devices such as fractional flow reserve, right heart catheterisation, left ventricular angiography, arterial access/history of bypass surgery and vessel(s) treated), fluoroscopy time and operator.
Measurement of scattered radiation
Dosimetry is performed in the presternal region, outside the lead apron, with a Personal Dosimeter (Radex One). Both the first and second operators wear the dosimeter. All procedural decisions are left to the operators' discretion, the measurements do not interfere with clinical routine except for the radiation protection device used and they do not affect patients' safety.
Dosimetry data are entered in duplicate in paper and in an excel database. Duplicate measurements were performed before initiation of enrolment and are performed at regular (2 months) intervals to guarantee the quality of the measurements. Physicians were trained at the beginning of the study on how to use the dosimeters; their compliance with study procedures and the correct use of the dosimeters is controlled daily. Data entry is audited at weekly intervals. Patient dosimetry is not performed.
Randomisation and blinding
Consecutive coronary procedures are randomised. Randomisation is done in a 1:1:1 ratio using blocks (each block 30 exams) without stratification. A randomisation list was generated by means of Medcalc (Mariakerke).
Allocation concealment
In order to minimise selection bias, the randomisation list is kept by the nurses, who prepare the corresponding radiation device for each procedure. Since patients are seen before catheterisation by the physicians only, this reduces the possibility that the randomisation scheme is subverted by the investigators.
Selection and withdrawal
Recruitment
No patient is directly enrolled in this study; measurements of scattered radiation are performed during normal routine and they do not interfere with patients' diagnosis or therapy. A total of ~1000 exams per catheterisation laboratory are performed yearly in our centre (elective exams conducted during normal working hours).
Consecutive procedures will be randomised.
Withdrawal criteria
There is no withdrawal criterion. All procedures will be enrolled consecutively.
Informed consent
The protocol was approved by the ethics committee of the local Landesärztekammer. Since all measurements are performed during clinical routine, the treatment is not influenced by the measurements, and all patient data are saved in an anonymous way, the ethics committee issued a waiver for the collection of patients´ informed consents (reference number 2018–13051-KliFo).
Statistics
Details of the statistical analysis of the data collected in this trial will be documented in a Statistical Analysis Plan (SAP) that will be generated and finalised before closing the database. The SAP is based on the protocol including all amendments. The document may modify the plans outlined in this protocol; however any major modifications of the primary endpoint definition and/or its analysis will also be reflected in a protocol amendment. Any deviation from the original statistical plan must be described and justified in the final report. The statistical analysis will be conducted by means of Medcalc V.9.2.1.0. The investigator and the sponsor, and their delegates, will have unrestricted access to the dataset.
The primary analysis of the study is the difference among the three groups, which will be tested using one-way analysis of variance based on the assumptions below. For comparison of the three separate treatment arms, we will use an ordered test strategy23 24: curtain and drape will be tested separately versus shield by a one-sided t-test for independent samples at a nominal level of 0.0125. This assures a multiple level of 0.025 by virtue of the Bonferroni correction method. If at least one of the two null hypotheses is rejected, the two interventional arms will be tested for difference by a two-sided t-test at a significance level of 0.05. The final analysis will be performed using analysis of variance or a Kruskal-Wallis test based on the inspection of the Q-Q plots.
The association of operators´ exposure with all variables described under ‘secondary objectives’ will be tested using univariate and multivariable regression analysis. All parameters showing a p<0.10 in univariate analysis will be entered in the multivariable analysis.
The sample size calculation is based on the following assumptions:
A two-tail α=0.05
β=0.10
Relative exposure of 6.0±5.0 μSv/cGy/cm² in the shield (control) group (based on historical data from our laboratory).
Mean difference between groups=1.0 μSv/cGy/cm², that is, an expected relative exposure of 5.0±5.0 μSv/cGy/cm² in the curtain and 4.0±5.0 μSv/cGy/cm² in the drape group. With these assumptions, a sample size of 480 measurements would be necessary. We aim to recruit a total of up to 700 procedures to allow investigation of possible interactions beyond the primary analysis, for instance whether the additional protection devices are only important in patients with BMI above 30, in interventions versus diagnostic procedures, or in longer versus shorter procedures.
Analysis populations
All procedures which are assigned a randomisation number are considered as enrolled/randomised procedures, even if the radiation protection device is not applied.
Since the study does not affect patients’ privacy, well-being or treatment, there is no safety population.
Efficacy analyses
Primary analysis will be based on an intention to treat analysis set, containing all procedures which were randomised.
Safety analyses
The procedures related to the study do not interfere with normal routine in the catheterisation laboratory. Therefore, there is no risk for the patients, and no measurement is performed on the patients directly.
Confidentiality
The subjects´ name and other personal information is not recorded. The operator’s name is recorded with his/her consent.
Ethics
The procedures set out in this trial protocol, pertaining to the conduct, evaluation and documentation of this trial, are designed to ensure that all persons involved in the trial abide by good clinical practice (GCP) and the ethical principles described in the Declaration of Helsinki. The trial is carried out in keeping with local legal and regulatory requirements. The requirements of the Arzneimittelgesetz, the GCP regulation, and the Federal Data Protection Law are kept. Since measurements do not affect patients´ diagnosis, treatment, or in any way pose a threat to their health, and no personal information is collected, the ethics committee has agreed that no informed consent is necessary.
Patient and public involvement
Since the outcomes of the study refer to X-Ray exposure in medical staff, patients are not expected to profit directly from the results of this trial. Patients were therefore not directly involved in the planning of the study nor are they affected by study measurements. No patient adviser was involved. Study participants are physicians, co-authors of the research. We plan to publish the results in an international journal to disseminate the results.
Audit
Competent authorities and sponsor authorised persons (auditor) may request access to all source documents, CRF, and other trial documentation in case of an inspection or audit. Direct access to these documents will be guaranteed by the investigator who will provide support at all times for these activities. Source data documents can be copied during inspection or audit after the identity of the subject have been made unrecognisable. No external audits are planned for this trial.
Potential conflicts of interest
The trial is funded by the Kardiologie I, University Medical Centre Mainz. No manufacturer of the drugs has been involved in this study. None of the authors has conflicts of interest to declare.
Dissemination
Publication resulting from the study shall require the approval of the co-authors. The results of the trial will be published as original article(s) in medical journals and/or as presentation at congresses. The principal investigator is senior author of the article. He or his delegates will present the data at appropriate congresses. The choice of the journal for the publication will be made by the principal investigator in agreement with the co-authors. Besides the Principal Investigator, a substantial contribution to the recruitment of subjects, a substantial contribution to interpretation of the data and/or a substantial contribution to drafting the article or revising it qualify for authorship. Source data will be made available on justified request.
Insurance
There is no insurance.
Limitations
Given the large variability in radiation among procedures and patients and the parallel design, it is possible that differences in radiation exposure as well as procedure types will be inhomogeneously distributed among groups. As well, we expect a wide variability in fluoroscopy use and radiation based on the spectrum of cases (from diagnostic angiograms to complex interventions). This variability reflects day-to-day clinical practice for interventional cardiologists and will be addressed in post-hoc analyses. Radiation exposure is measured at chest level (outside the lead apron) since this is the most accessible region and the one that least interferes with clinical routine. Exposure under the apron and at the level of neck, eye or hand is not assessed.
Dosimetry at patient level will also not be measured. Total administered radiation (DAP, dose-area product) will be used as a surrogate of patient dosimetry.
Finally, there is no control group without shield and no blinding was possible. This would however have exposed the staff to radiations and would have therefore been ethically and practically unacceptable.
Study committees
The steering committee of the study is composed by the senior and junior author, who have the responsibility for the ethical conduct of the study and for the accurate collection of data by the study nurses. This study does not involve clinical outcomes, there is no adjudication committee or Data safety and monitoring board.
Trial status
Data acquisition is ongoing. The first patient was included in August 2018. We expect the study to be closed in December 2019.
References
Footnotes
Contributors The authors have provided intellectual input for the design and planning of the study. The manuscript and protocol were initially written by RA and TG, and were corrected and edited by MB, NM, MK, MA, MG, DqK, PW, TM. All the authors approved the final version.
Funding The senior author is DZHK (Deutsches Zentrum für Herz und Kreislauf Research) professor. University Medical Centre of the Johannes Gutenberg-University Mainz.
Competing interests None declared.
Ethics approval The protocol was approved by the ethics committee of the local Landesärztekammer (2018 – 13051 -KliFo).
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.