Article Text

Abstract
Introduction Adolescents and youth living with HIV (AYLHIV) have lower retention in care, adherence to treatment, and viral suppression compared with adults. Stepped care is a process by which clients are assigned to increasingly intensive services or ‘steps’ according to level of need. Differentiated care, in which stable clients access less frequent services, can be combined with stepped care to align needs and preferences of youth to promote optimal engagement in care.
Methods and analysis This hybrid type I effectiveness implementation cluster randomised trial aims to evaluate a data-informed stepped care (DiSC) intervention for AYLHIV. AYLHIV ages 10–24 receiving care at 24 HIV treatment facilities in Kisumu, Homabay and Migori counties in Kenya will be enrolled. Twelve facilities will be randomised to the DiSC intervention, and 12 will provide standard care. A clinical assignment tool developed by the study team will be used at intervention sites to assign AYLHIV to one of four steps based on risk for loss to follow-up: differentiated care, standard care, counselling services or intensive support services. The primary clinical outcome is retention in care, specifically missed visits (failure to return within 30 days for any visit) and 12-month loss to follow-up. Implementation outcomes are based on the Reach, Effectiveness, Adoption, Implementation and Maintenance framework. Proportions of missed visits will be compared using mixed effect models clustered by facility and participant.
Ethics and dissemination This study has been approved by the University of Washington Institutional Review Board (STUDY00011096), Maseno University Ethical Review Committee (MUERC/00917/20) and the Kenya National Commission for Science, Technology and Innovation (444824). AYLHIV provide written informed consent when legally permitted, or assent with caregiver permission for minors. Study staff will work with a Community Advisory Board, including youth members, to disseminate results via discussions, presentations, journal publications and local or international conferences.
Trial registration number NCT05007717.
- HIV & AIDS
- Community child health
- Quality in health care
- Paediatric intensive & critical care
- Clinical trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- HIV & AIDS
- Community child health
- Quality in health care
- Paediatric intensive & critical care
- Clinical trials
Strengths and limitations of this study
Use of a data-driven approach to match adolescents and youth living with HIV to services according to need.
Includes implementation outcomes to account for context that will optimise both intervention approach and sustainability.
Integrates validated survey scales with routinely collected electronic medical records data to assess outcomes.
Overlap between standard of care and the intervention steps may limit ability to detect a significant difference in outcomes.
May be subject to routine care interruptions such as strikes, stock outs, the COVID-19 pandemic and workforce turnover that could undermine the intervention.
Introduction
An estimated 88% of youth, including adolescents and youth living with HIV (AYLHIV) reside in sub-Saharan Africa.1 Worldwide, 410 000 youth between the ages of 10 and 24 were newly infected with HIV in 2020, and perinatally infected children of the last decade are ageing into adolescence.1 Compared with adults, youth have lower retention in care, adherence to antiretroviral therapy (ART) and viral suppression,2–8 increasing the risk of HIV transmission and disease progression.9 10 AYLHIV frequently fail to achieve viral suppression11 12 with approximately 30% experiencing non-suppression or failure after 12 months on ART.13–17
Test and Start models, where individuals living with HIV are rapidly initiated on treatment, address loss to follow-up in the pre-ART period, with early evidence of success.18 However, there are fears that increasing caseloads, interlinked burdens of disease, sudden epidemic outbreaks and other emerging health challenges will add to healthcare worker (HCW) burdens in already strained healthcare systems.1 Differentiated models of service delivery have been proposed as a client-centred approach that simplifies and adapts HIV services across the cascade to better serve those in care and reduce unnecessary burdens on the health system.19 However, due to poor retention outcomes, Kenyan guidelines classify all adolescents as ‘unstable’.20 Thus, AYLHIV are currently not able to access differentiated approaches, including community-based refills or longer refill durations, which may benefit this population and free up HCW time to provide more intensive care to youth in need.
Stepped care models, a process by which clients are assigned to intervention steps according to level of need, have been used in mental health fields to organise provision of services; and to support clients, HCWs and caregivers to identify the most effective interventions.21 Models typically start with a low-intensity, evidence-based treatment and systematically progress to higher levels of care or intervention as clients fail to respond.22 Early studies suggest that stepped care approaches improve access to care, client outcomes and programme efficiencies, including client volume.23–25 A key feature of stepped care is outcome monitoring, giving both clients and HCWs feedback to inform care options and service delivery.
One challenge with retention interventions is the ability to identify clients who need more intensive services before they are lost to follow-up. Clinical prediction tools classifying individuals into high and low-risk groups have potential to identify those in need of intervention and support more efficient service delivery prior to poor outcomes occuring.26–29 Studies using these tools among key populations in the USA26 29 and studies in Kenya28 30 found clinical characteristics that were predictive of HIV acquisition. Similarly, tools using a minimal number of variables have been shown to predict virologic failure or mortality in adult cohorts in both the USA31 and low resource settings.31–33 A prediction tool for loss to follow-up could support HCWs to better identify youth at risk for missed visits, rather than waiting until loss occurs, and be used to assign youth into appropriate steps of service delivery. This study aims to evaluate a data-driven, stepped care intervention assigning AYLHIV in Kenya to differentiated or more intensive service steps.
Methods and analysis
Study design
This hybrid type I effectiveness implementation parallel cluster randomised trial aims to evaluate the effectiveness and implementation of a data-informed stepped care (DiSC) intervention for AYLHIV in Kenya. We hypothesise that the DiSC intervention will result in better retention in care and viral suppression among AYLHIV in intervention sites compared with those in control sites. We hypothesise that the DiSC intervention will be integrated into routine AYLHIV service in a way that is feasible and acceptable for HCWs, reaches a high proportion of youth attending facilities and is able to be implemented with fidelity. Focus group discussions and in-depth interviews will support qualitative understanding and optimisation of study implementation.
Study sites and population
We will conduct this study at 24 HIV care facilities located in Kisumu, Homabay and Migori counties in Kenya. Eligible facilities include those with ≥100 AYLHIV enrolled in care, a functioning electronic medical records (EMR) system and interest in participating. Eligible AYLHIV are ages 10–24 and enrolled in HIV treatment at participating clinics. AYLHIV who are not aware of their HIV diagnosis will be excluded. We aim to enrol a minimum of 50 AYLHIV per site, up to a maximum of 6000 AYLHIV total.
Patient and public involvement
Grounded in the concept of the stepped care model used in mental health, the DiSC intervention was developed through a combination of: (1) review of stepped care practices in the USA, (2) preliminary data from a longitudinal cohort of >1300 AYLHIV in Kenya and (3) a modified user-centred design (UCD) workshop with key stakeholders (AYLHIV, youth leaders, national and county health officials, HCWs and caregivers of AYLHIV). Cohort data were used to characterise the AYLHIV population and develop a clinical prediction tool for loss to follow-up to aide providers in assigning AYLHIV to care steps. These data, alongside information on stepped care, differentiated care policies, best practices for adolescent care, national guidelines and existing services in clinics in the catchment area, were presented to stakeholders at the UCD workshop. Given COVID-19 social gathering restrictions, the workshop included a series of small group meetings followed by a large group meeting, where participants discussed which services would be appropriate for each step, aligning current practices in facilities. Participants were encouraged to develop the most inclusive and simplest service allocation approach that would work in the largest number of facilities in Kenya. Following the workshops, the study team refined the clinical prediction tool and intervention steps based on the feedback of stakeholders.
Conceptual framework
This study uses a socio-ecological framework to understand adolescent care-seeking behaviours and is broadly informed by Andersen’s model of health service use34 and elements of Pantin’s eco-developmental theory.35 Andersen’s model describes how environmental factors, including the health system, interact with population factors to motivate individual uptake of health services. The developmental perspective in Pantin’s theory further suggests that these factors and relationships change during transition to adulthood. From a theoretical perspective, the stepped care model is grounded in Stages of Change Theory, tailoring different levels of care intensity to different stages of health behaviour change.36
Intervention components
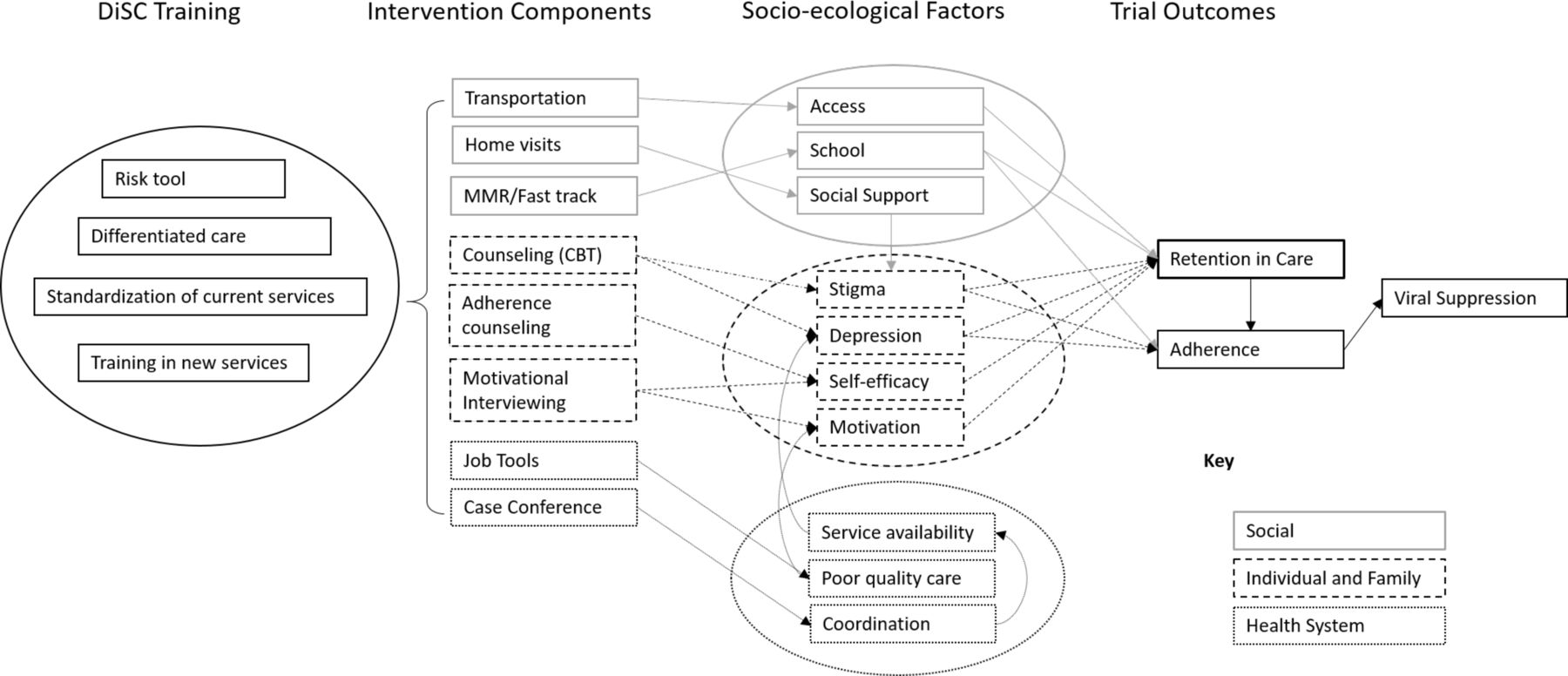
The DiSC intervention uses a clinical assessment tool, based on the original prediction tool, to assign AYLHIV to different levels—or steps—of care based on their health and psychosocial needs. As those with lower needs becomes eligible for less frequent contact, this allows more HCW time to concentrate on providing more intensive services (figure 1). In addition to reinforcing standard of care elements, the intervention also includes HCW training of cognitive behavioural therapy (CBT) and motivational interviewing. These core components address social (transportation, school, social support); individual and family (stigma, depression, self-efficacy and motivation); and health system factors (service availability, quality of care, care coordination) as a holistic approach to promote retention, adherence and ultimately viral suppression.

{kind=link}
Model of the intervention. CBT, cognitive behavioural therapy; DiSC, data-informed stepped care.
Intervention procedures
At enrolment and at every visit, HCWs will use the assessment tool to determine risk level and assign AYLHIV to a care step. Information will be obtained through self-report and HCW review of the medical record. The tool uses a combination of key loss to follow-up predictors and Kenyan national guidelines to match AYLHIV to one of four steps: differentiated care, standard of care, individual counselling or intensive support (table 1).
Intervention steps
At the lowest step, AYLHIV who adhere well to treatment with no missed visits or health concerns will be assigned to receive differentiated care services, including multi-month refills, longer visit intervals and/or fast-track visits. AYLHIV with health concerns (pregnancy, opportunistic infections or TB) or those newly enrolled in care will be assigned to the second step, receiving standard care under Ministry of Health guidelines. AYLHIV with a history of missed visits in the past 6 months or depressive symptoms on standardised Patient Health Questionnaire-2 (PHQ-2) depression screening will be assigned to the third step, individual counselling. Within that step, those with a history of missed visits will receive one motivational interviewing session, and those with depressive symptoms will receive four CBT counselling sessions and referral to further mental health evaluation and treatment where warranted. The last step, intensive support, includes AYLHIV with unsuppressed viral load (VL). They receive services from steps 2 and 3 as needed, and enhanced adherence counselling with case management services such as home visits or transportation support as needed. The study team will guide facility-based quality improvement at intervention sites to monitor unsuppressed clients and support timely return of VL results. Control sites will continue with standard care for AYLHIV clinic visits according to national guidelines.
Recruitment and retention procedures
The sampling frame includes 55 clinics in three high-burden counties in Western Kenya. Among those, 24 clinics that meet eligibility criteria have the highest youth enrolment, and whose leadership is willing to participate will be selected and randomised to intervention or control. AYLHIV in participating facilities who are aware of their HIV status will be identified by facility providers and referred to the study team for eligibility screening and consent. A standard recruitment script with talking points will be used. Recruitment will be conducted during different days and times of the week, during at least two school breaks and ‘youth friendly days’ to maximise enrolment. AYLHIV at intervention sites will be consented for participation in the DiSC intervention and longitudinal surveys. Control sites will be consented for longitudinal surveys only. AYLHIV participants will have 12 months of follow-up time.
Randomisation and blinding
A total of 24 clinics will be randomised in a 1:1 ratio using computer generated random numbers to either intervention or control, using restricted randomisation to balance county representation and facility volume, aiming to balance these variables between arms. Randomisation will be done prior to study initiation at the University of Washington by a biostatistician not involved in study procedures. A list of clinics with their allocation arms will be sent to the study team. The intervention is administered at the clinic level; thus, it is not possible to blind participating clinics or study team members.
Outcome measures
The primary outcome is retention in care, measured as both the proportion of missed visits 1 year after enrolment, and the proportion of AYLHIV who became lost to follow-up with no subsequent return to care during the study period (table 2). Secondary outcomes are viral non-suppression, defined as HIV VL >1000 copies/mL; receipt of differentiated services (multimonth refills or fast-track visits); and ART adherence defined as a remaining pill count<80% (estimated by days used and inter-visit interval).
Study outcomes and data sources
Implementation assessment includes barriers, facilitators, and adaptation strategies of intervention implementation. Outcome measures use the Reach, Effectiveness, Adoption, Implementation and Maintenance framework.37 We will routinely evaluate the proportion of youth enrolled in the intervention (Reach), the proportion of trained HCWs using the intervention (Adoption), proportion of youth assigned to correct step (Fidelity), proportion of youth exposed to correct services in each step (Fidelity), types of HCW adaptations made for optimising delivery (Implementation) and the proportion of facilities using the intervention tools at study end (Maintenance) using study-specific case report forms (table 3). We will also evaluate HCW perceptions of acceptability, feasibility and appropriateness of the DiSC intervention.38 39
Implementation outcomes
Data collection
We will abstract AYLHIV medical record data at baseline, and every 6 months. Data from all enrolled AYLHIV with at least one clinic record within the 12 month period prior to the first data abstraction date will be included. Data will be abstracted at the facility or at the office of the technical partner that supports the EMR system at the facility. The EMR system captures data on client anthropometric measures, demographics, HIV testing history, clinical history, ART adherence data, laboratory data, CD4 count, transfers and discontinuations. If EMR data are unavailable, paper records will be abstracted using mobile REDCap, which enables automatic upload of data to a secure, password-protected study server. Routine HIV VL testing (done 6 months after ART initiation, then annually) will be abstracted from the Kenya National AIDS & STI Control Program database.
Youth surveys will be administered by study staff following intervention assignment by the HCW. Surveys include questions on sociodemographic,40 healthcare use, stigma,41 sexual behaviour and violence using questions adapted from the WHO Multi Country Study,42 social support by the Multidimensional Scale of Perceived Social Support,43 depressive symptoms by PHQ-9),44 anxiety by General Anxiety Disorder-7,45 resilience by Connor-Davidson Resilience Scale-2,46 self-efficacy,47 personal health knowledge, HIV disclosure, and medication adherence by HIV Treatment Adherence Self-Efficacy Scale.48 Surveys will be administered every 6 months either in-person or over phone by a trained study staff. Survey visits will coincide with clinic visits whenever possible. At the end of the study, additional surveys will be given to a random sample of youth and caregivers in intervention sites to evaluate satisfaction with care. We will also conduct in-depth interviews (IDIs) or focus group discussions (FGDs) with youth in intervention sites to determine acceptability, feasibility and satisfaction with the intervention.
Facility managers will complete baseline and annual facility surveys to understand baseline resource capacity to implement future interventions and modifiable and non-modifiable health system factors. Variables will include availability of youth-friendly services, management and referral systems, and differentiated care services available. We will conduct pre-trial surveys with HCWs to assess structural readiness for implementation39 and intervention beliefs about acceptability, feasibility and appropriateness of intervention implementation. During the first 6 months of the trial, HCWs will participate in twice-monthly continuous quality improvement (CQI) meetings using plan-do-study-act processes to assess specific adaptations that optimise reach, adoption, fidelity, acceptability and feasibility. Prior to each meeting, HCWs will complete surveys to evaluate changes in implementation. We will conduct FGDs with HCWs in intervention sites at 6 months post-intervention implementation, and FGDs, IDIs and surveys with HCWs post-trial to determine experiences with the DiSC intervention and evaluate barriers and facilitators of intervention utilisation. All FGDs and IDIs will be guided by the Consolidated Framework for Implementation Research.49 50
Sample size calculation
We estimate that participating facilities will have an average of 100–200 AYLHIV in care per clinic. Based on preliminary data, we assume that 75% will remain in care by the end of the 12-month follow-up period. Assuming 12 facilities per arm, α=0.05, a two-sided test, and a coefficient of variation of 0.10, we have 80% power to detect a 14% difference (75%–89%) with ≥150 AYLHIV per facility, and a 15% difference (75%–90%) with ≥50 AYA per facility. Assuming a coefficient of variation of 0.15, we have 80% power to detect a 17% difference (75%–92%) with≥50 AYLHIV per facility.
Statistical methods and analysis
Characteristics of facilities randomised to each arm will be summarised using descriptive statistics. The proportion of missed visits will be compared between study arms using mixed effect models clustered by facility and participant. Time to loss to follow-up will be compared between arms using survival curves and Cox proportional hazards regression, with censoring of deaths or transfers. Proportions of secondary outcomes (viral non-suppression, differentiated care, adherence) will each be compared between study arms using mixed effect models clustered by facility and participant. Exploratory sub-group analyses for missed visits and loss to follow-up will be performed by gender, age-group and step assignment groups. Facility factors including concurrent adolescent-friendly services and high/low performance will be evaluated as moderators of intervention effectiveness. Pre-trial and post-trial survey data will be summarised to evaluate frequencies, variability and associations. Adaptations made to the intervention during the CQI process will be categorised using the Framework for Reporting Adaptations and Modifications Expanded,51 and compared with variations in implementation outcomes to identify modifications associated with sustained improvements in implementation. Qualitative data will be analysed using a combination of thematic52 and directed content analysis53 approaches to characterise the determinants of implementation success and explore personal experiences with the DiSC intervention.
Ethics and dissemination
This study has been approved by the University of Washington Institutional Review Board (STUDY00011096) and Maseno University Ethical Review Committee (MUERC/00917/20). Protocol modifications will be submitted to both committees. Youth participants will provide written informed consent for study procedures as permitted by law; youth without capacity to consent will provide assent while their caregivers will give consent unless exempted by the two ethics bodies. A sample consent form is provided in the online supplemental appendix. The trial will be monitored by a Data Safety and Monitoring Board (DSMB), as well as by external monitors appointed by the funder. Severe adverse events will be monitored and reported to the DSMB and study monitors in real time. All data will be kept confidential and de-identified by the data manager. Consent documents will be kept separate from study data and secured in a locked cabinet.
Supplemental material
Study staff will work with a Community Advisory Board, including youth members, to disseminate results to participants and the community via discussions and presentations. We will further disseminate findings through journal publications and local or international conferences. Data will be submitted to the National Institute of Child Health and Human Development (NICHD) Data and Specimen Hub (DASH) no later than 1 year after acceptance of the primary manuscript or study closure, whichever comes first.
The trial is registered at ClinicalTrials.gov, NCT05007717. Enrolment took place 19 April to 19 July 2022; the trial will conclude by 31 July 2023.
Discussion
This study is part of the Prevention and Treatment through a Comprehensive Care Continuum for HIV-affected Adolescents in Resource Constrained Settings (PAT3CH) consortium, a NICHD-funded international group of combination individual, family, community, structural and health system intervention studies to improve health outcomes among adolescents and youth at risk for or living with HIV.54 Our study aims to evaluate a stepped care intervention to tailor service delivery according to AYLHIV needs and ultimately improve retention in care and other clinical and psychosocial outcomes. The intervention has been developed based on a theoretical foundation and informed by pilot data and stakeholder input.
Our multicomponent intervention is based on a combination of evidence-based interventions and recommended but untested strategies to clearly allocate services using a pre-specified algorithm/tool to tailor specific services for AYLHIV.55–59 Services include individual motivational interviewing to preemptively improve retention, CBT to address depressive symptoms, and enhanced counselling for adherence. System improvements include facility quality improvement and guideline refreshers. Together, these intensive individual and system-level interventions as elements of higher steps address current gaps in care including resources for mental health treatment60 and a breakdown in action on unsuppressed VL results.61 One way our approach differs from US-based stepped care interventions is that we include risk for non-retention, rather than waiting for non-retention outcomes alone, to assign AYLHIV to steps.
The use of a data-driven tool to identify AYLHIV at highest risk of loss to follow-up is consistent with stepped care principles of using routine data to inform care needs. The risk assessment provides a systematic way to identify AYLHIV who are most likely to be safe to initiate on differentiated services, despite being classified by Kenya’s MOH as a high-risk group overall. Currently, differentiated services like longer visit intervals are only applied to stable adults, due to concerns that AYLHIV may not be able to sustain adherence and retention without more frequent contact. Our approach will emulate adult standards for differentiated care in terms of identifying eligible AYLHIV. Data from this study will provide important evidence for Ministries of Health who seek to extend differentiated care to AYLHIV. Simultaneous measurement of implementation outcomes throughout the trial will help to determine best practices to ensure sustainability and inform issues of setting and context, which may contribute to eventual scale-up if the intervention is found effective.
This trial has limitations. Elements of several care steps are offered in control settings, which may limit our ability to detect a difference between intervention and control arms, and there is a possibility of transfer of enrolled clients between facilities. The study is operating through routine care programmes in Kenya, which are subject to strikes, stock outs, the COVID-19 pandemic, and workforce turnover and may undermine fidelity of the intervention over the study course. Furthermore, the age range represents a heterogeneous group of AYLHIV, and our sample size may limit our ability to detect differences in effectiveness among key subgroups. Finally, there are social factors that influence AYLHIV uptake of services and may not be addressed within the health system alone.
In summary, this a data-driven, provider-led, health system intervention aims to identify young people most at risk for loss to HIV care, sub-optimal adherence and viral failure. Our stepped care approach, combined with a clinical prediction tool, is a timely and flexible intervention in the context of differentiated care and numerous ongoing care initiatives. By improving engagement in care and optimising provision of limited resources, this intervention may ultimately improve health among adolescents and youth in Kenya and provide support for testing stepped care approaches in other settings.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PK, GJ-S and KA are principal investigators. PK, GJ-S, KA, BAR and KB-S designed the study and supervised trial protocol development; IN, JD, WJ, SS, II, NC and JB contributed to the study protocol. BAR and WJ were responsible for statistical design; KB-S and NC were responsible for implementation science approaches. PK drafted the initial manuscript and all authors critically revised, read and approved the final manuscript.
Funding This work was supported through the PATC3H consortium, funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under grant UG3/UH3 HD096906.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.