Article Text

Abstract
Introduction The development of paediatric medical devices continues to lag adult medical devices and contributes to issues of inequity, safety, quality and patient outcomes. New legislation and funding mechanisms have been introduced over the past two decades, but the gap remains. Clinical trials have been identified as a pain point, but components of effective clinical research infrastructure are poorly understood. As part of a multimodal research strategy, the Pediatric Device Consortia (PDC) will conduct a scoping review to better understand infrastructural barriers to and facilitators of paediatric medical device clinical research identified in the health sciences literature.
Methods and analysis The following databases will be included for this review: Medline, Embase, Cochrane CENTRAL, Web of Science and IEEE Xplore. Additional grey literature will be sought out through Google Scholar and reviewing the citations of included studies. Included studies will discuss medical devices according to the U.S. Food and Drug Administration classification, focus on the paediatric population (ages 0–21 years) and involve human premarket or postmarket research. All study types that were published in 2007–present in English, Spanish, French or Italian will be included. Using Covidence web-based software, two independent reviewers will screen the resulting titles, abstracts and the full text of potential studies. Conflicts will be resolved by the primary investigator during both phases. REDCap will be used for quantitative and qualitative data charting, generating data tables and narrative synthesis.
Ethics and dissemination This research did not require research ethics board consideration as it does not involve human participants and all data will be collected from published literature. We will share our findings through peer-reviewed manuscripts, clinical and research conference presentations and professional networks available to the PDC.
Study registration Open Science Framework (https://osf.io/k72bn).
- Health policy
- PAEDIATRICS
- Clinical trials
- Health Equity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This scoping review is a novel examination of the paediatric medical device clinical infrastructure with potential to impact policy and practice.
The team adhered to scoping review methodology standards including the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension statement and the Joanna Briggs Institute Manual for Synthesis scoping review chapter.
While the team will be able to include studies in English, Spanish, French and Italian, potentially relevant studies in other languages will not be included.
Through collaboration with subject experts and a medical librarian, an exhaustive search has been conducted, but it is still possible given how the paediatric literature is documented and the indexed and the overabundance of medical devices and categories that potentially relevant studies may not have been discovered and included.
Introduction
Medical devices, especially those that require clinical validation, are strictly regulated products intended to diagnose, cure, mitigate, prevent or treat diseases that, unlike drugs, do not achieve their primary function through chemical action or by being metabolised (Section 201(h) Food Drugs and Cosmetics Act). The dearth of medical devices designed and tested specifically for children is a significant health inequity that creates issues relating to safety, quality and patient outcomes.1 Numerous barriers hamper progress in the paediatric medical device field.2 The most notable challenges could be grouped into four major categories: (a) Ethical barriers: investigations with children as the vulnerable population are considered to be more risky than with adults; simultaneously children cannot fully understand these risks and thus give an informed consent to participate in research; (b) Clinical barriers: unlike adults, children’s physiology and anatomy drastically changes over time which requires innovative technological solutions to accommodate, for example, miniaturisation or adaptability; additionally, children may not have the cognitive capacity to interact with or operate medical technology; (c) Regulatory barriers: smaller sample size and age heterogeneity within the paediatric population renders reliable safety data difficult to obtain; meanwhile, the regulatory agencies have a higher standard for paediatric device approvals; (d) Financial barriers: due to a small market size, bone fide paediatric medical device innovators struggle to procure venture capital funding necessary to support device development; even if successful, the device reimbursement rates are lower in paediatrics and no standardised national coverage exists.2 Although federal agencies like the National Institutes of Health (NIH), the Food and Drug Administration (FDA) and Centers for Medicare and Medicaid Services are responsible for discrete tasks like funding device–related research, regulating devices and guiding device reimbursement, there is no national infrastructure to support and organise systems-level solutions to these problems. As a result, paediatric medical device development lags adult devices by as much as 10 years.3
The Pediatric Device Consortia (PDC) Programme is an FDA initiative established by Congress in 2007 to fund non-profit consortia that promote and guide the development of paediatric medical devices through a number of key activities, including consulting with subject matter experts, establishing new research and clinical partnerships and providing non-dilutive funding.4 Across four grant cycles, the FDA has awarded 23 consortia grants that have collectively supported over 1000 paediatric medical device projects across the USA.5 In 2021, the currently funded PDCs received supplemental funding to evaluate the challenges associated with conducting paediatric medical device trials and potential solutions for improving associated infrastructure. As part of a multimodal research strategy to describe barriers and identify possible solutions, we are undertaking a scoping review to understand what is currently known about paediatric medical device research infrastructure and potential best practices.
Rationale
Improving the various research processes leading to the development of novel paediatric medical device technologies is one key component of addressing the gap in paediatric medical devices. Device research is significantly different from pharmaceutical research; is iterative by design and often requires collaborations between academia and industry.6 Research that involves children must also address a whole host of specific considerations and barriers.7 These factors and others create a high level of complexity that has not been amenable to some of the programmatic solutions that have been implemented for paediatric drug research, such as the NIH-sponsored Pediatric Trial Network.8 To date, very little is known about best practices or programmatic features that set up an institution to successfully support paediatric medical device research.
Methods and analysis
Our research team is composed of 14 industry, non-profit and academic professionals with expertise in healthcare and medical device innovation. The research team is led by the librarian (LK) who created a framework to facilitate research activities. On 16 October 2021, said librarian (LK) ran a preliminary search in PubMed (National Library of Medicine) using the Medical Subject Heading (MeSH) for ‘Device Approval’ which generated 3094 results. When this search was paired with the built-in filter ‘Child: birth-18 years’ the number of results dwindled to 131. This collection of paediatric citations did not include any systematic or scoping reviews. It did however include several literature reviews focused on a specific discipline9 10 or the FDA,11 12 along with a variety of editorial publications.1 13 When compared with medical device systematic and scoping reviews in the adult population,14–16 we found this lack of literature the appropriate justification for a well-conducted scoping review. Given the scoping review’s exploratory and iterative nature, we intend to seek out evidence of barriers to and facilitators of paediatric medical device clinical research and its associated infrastructure by thoroughly exploring both the traditionally and the non-traditionally published literature. We started with the population/concept/context framework developed and described by the Joanna Briggs Institute to develop our protocol and to inform search strategies and eligibility criteria.17
Stage 1: identifying the research questions
The objective of this scoping review is to provide an overview of the current landscape of paediatric medical device research during the clinical phase of development and propose a nationally applicable strategy to improve the associated infrastructure for conducting paediatric medical device trials. We are conducting this scoping review with two guiding questions (GQs):
GQ 1: What is known about current barriers to and facilitators of conducting paediatric medical device trials in the USA and abroad (for FDA harmonisation and comparison to American systems)
GQ 2: What are existing strategies to improve the associated infrastructure for conducting paediatric medical device trials?
While medical devices are critical to supporting the health and well-being of children, their development is severely limited by the clinical trials’ cost and time, with feasibility and pivotal studies costing on average $1.4 million and $30.7 million, respectively.18 Although the exorbitant cost of device development and validation is well known, we hypothesise that the complexities of these processes are either misunderstood by or unknown to both medical professionals and other critical stakeholders, which might exacerbate the required effort. Through this research, we hope to gain additional insight into technical, ethical and regulatory challenges that might prevent hospitals from engaging in paediatric research, delay participant recruitment, prolong clinical trial conduct and/or prevent its completion.3 19–21 Based on our preliminary searches and existing trends in limited paediatric research,22 23 we anticipate that we will find very few peer-reviewed publications that specifically focus on paediatric medical device research infrastructure. Nevertheless, we believe these findings taken together will allow us to elucidate factors contributing to the successful conduct of paediatric medical device studies and to offer a list of regulatory and legislative recommendations to inform the paediatric medical device policymaking.
Stage 2: identifying relevant literature
A medical librarian (LK) created Medline (Ovid) and Embase (Elsevier) search strategies (online supplemental file 1) using a combination of controlled vocabularies (MeSH and Emtree) and keywords for the concepts of medical devices, development and paediatrics. Team members reviewed the strategies and results to edit and improve the search strategy. With the approval of the team, the librarian will then create customised search strategies using controlled vocabulary (when available) and keywords in the following additional databases: Cochrane CENTRAL (Wiley), Web of Science (Clarivate Analytics) and IEEE Xplore (Institute of Electrical and Electronic Engineers). To capture grey literature, or non-traditionally published works, we will also search Google Scholar and include the first 200 results.24 Finally, we intend to screen the reference list of studies that are ultimately included following the full-text screening process.
Supplemental material
Stage 3: study selection
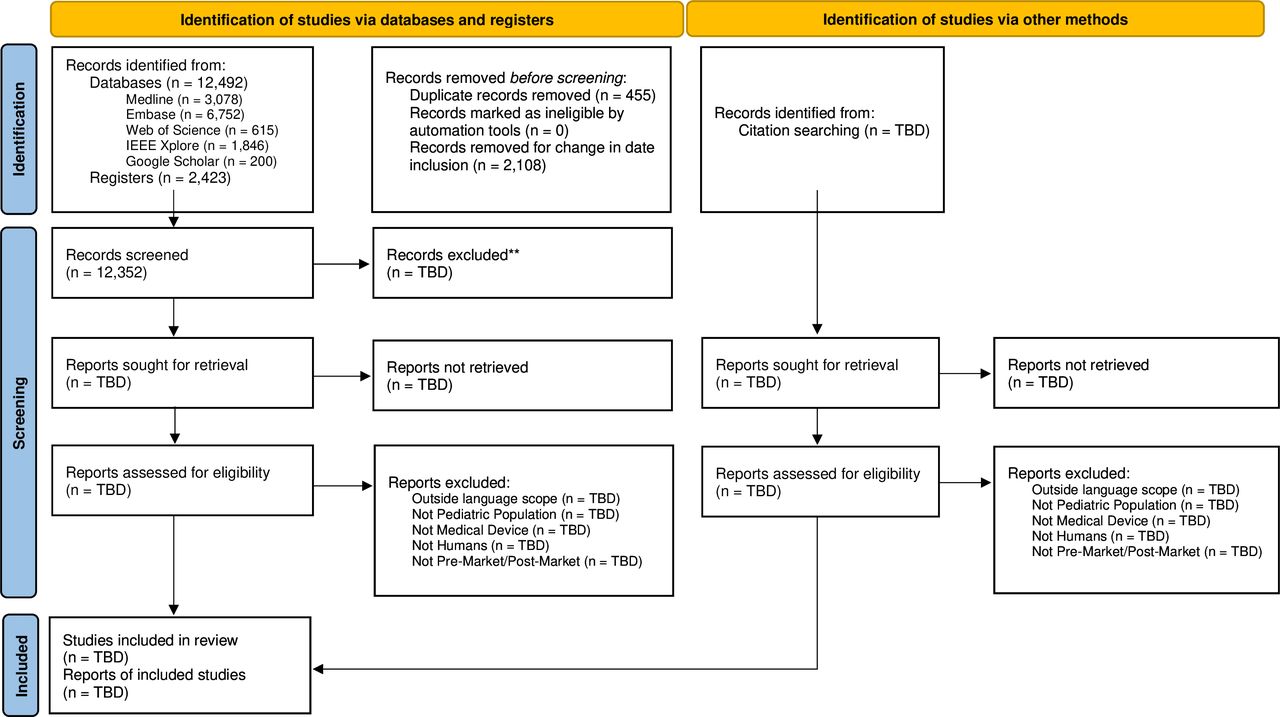
The resulting citations (n=14 914) from each database search have been exported into an EndNote V.20 (Clarivate Analytics: Philadelphia, Pennsylvania, USA) library and duplicates were removed.25 We created a Covidence Review (www.covidence.org 2022 Covidence v2960 c2c89313) and imported the de-duplicated collection of citations (n=14 537). The Covidence de-duplication software recognised an additional 39 duplicates and a total of 14 498 citations entered the title/abstract screening phase of the review. See figure 1 for the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for additional details.26 Using Covidence, two members of the title/abstract screening team (ATS, FJ, GZ, HK, JE, LK, LM, MC, PS and AS) will independently review each title/abstract based on the inclusion/exclusion criteria (table 1). Conflicts will be resolved by the primary investigator (JE). The same team will move forward with the full-text screening with two members independently reviewing each item and all conflicts will continue to be resolved by the primary investigator (JE).

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. The flow diagram depicts the flow of information through the different phases of the scoping review. TBD, To be determined.
Criteria for inclusion/exclusion of studies
Prior to starting the title/abstract screening, a core group of team members (CJK, FJ, JE, LK and UT) participated in a pilot screening where each participant independently screened the same set of 40 citations. This core group met and discussed all discrepancies and finalised the following inclusion criteria:
Population
The population includes potential paediatric-aged individuals as defined by the FDA as 0–21 years old to meet the review’s objective to focus on paediatric medical devices. We will include studies with a mixed paediatric and non-paediatric population if the authors include paediatric implications or discussion.
Concept
The concept includes medical devices as defined by the FDA, based on a three-tier risk classification (27; reviewed in detail in Espinoza et al 2): Class I (low-moderate risk), Class II (moderate-high risk) and Class III (high risk). We will also include other medical devices if they have been classified accordingly: Class III-like, combination, software as a medical device (SaMD) and digital health.
Context
The context must be the trial for development of the medical device including premarket and postmarket trials. We will exclude other types of trials such as marketing, clinical use, preliminary technological design and animal testing.
Types of evidence sources
We initially sought out to include studies published since 1999 to capture the impact of the FDA Modernization Act of 1997.28 However, after discussion with subject matter experts, the team decided to focus rather on the impact of the Pediatric Medical Safety and Improvement Act of 2007 which aimed to increase the availability of paediatric devices while also ensuring safety and effectiveness.29 By shifting our scope to studies published since 2007, we will both ensure an expedient and appropriately focused scoping review. Included studies must be published in English, Spanish, French or Italian given the language limitations of our scoping review team. We will include studies regardless of the setting or location of the authors or publication type. This inclusivity will allow us to compare the impact of medical device legislation and policies from different countries and attempt to effectively document the diverse landscape of relevant literature.
Stage 4: charting the data
A data charting form will be created using the REDCap electronic data capture browser-based software (Vanderbilt University: Nashville, Tennessee, USA)30 31 based on the drafted data charting tool (table 2). We will collect information about the age of the population discussed and the class and medical specialty of the device included. For the context, we will prioritise barriers and facilitators and capture them in the following categories: financial, regulatory, legislative and technical. Relying on the iterative nature of the scoping review methodology, we will initially create free-text descriptions of the devices and any proposed solutions. Once completed, we intend to complete a thematic analysis to organise and identify trends. Lastly, we will chart information about included studies to allow for comparison between publication types. All data charting members of the team will participate in pilot testing of the data charting tool by independently reviewing the same set of five papers. The group will compare results and discuss any discrepancies and revise the data charting tool accordingly. Two independent data charting members will complete the REDCap form for each of the included papers. Conflicts will be resolved through discussion among data charting members. We intend to rely on the iterative nature of the scoping review methodology as described by the Joanna Briggs Institute Manual of Evidence Synthesis.32 Consistent with that notion, our data charting form is not yet complete and we anticipate our process evolving throughout the data charting process.
Data charting form
Stage 5: collating, summarising and reporting the results
To ensure transparency and adherence to the established guidelines, we will follow the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist and explanation for reporting study findings.33 As part of this process, we will include the PRISMA flow diagram to document identified references, stages of screening and reasons for exclusion. Our scoping review will include a comprehensive list of all included studies in table 1. This table will contain key characteristics of the studies, including, but not limited to aims, population, methodology, device class, clinical areas of device use and key findings. We will use both the qualitative (content and themes) and quantitative (frequencies and percentages) data to report on the barriers to and facilitators of the development of paediatric medical devices described in the literature. The data will be visualised through diagrams and organised by device class and potential areas of device use, and we will report on the frequency of each identified barrier and facilitator, including the statistical analysis. To ensure the relevance and applicability of our findings, we will categorise the barriers and facilitators discovered in the data charting phase (step 4) to inform stakeholders from the private, academic and government sectors. In addition, we will compare traditionally published studies to grey literature as well as paediatric medical device trials to reviews and editorials. We recognise that the scoping review methodology is iterative, and we are prepared to make modifications to the data presentation should additional information become relevant. Ultimately, our goal is to provide a clear and comprehensive summary of all relevant literature on the paediatric medical device clinical trials to inform future research and development, guide regulations and policy, and assure patient safety.
Patient and public involvement
None.
Ethics and dissemination
Approval from a research ethics board was not required as the present study does not involve human participants or unpublished secondary data. Our target audiences include all individuals and organisations that play a role in paediatric medical device infrastructure across organisations and disciplines including healthcare, engineering, regulation, public policy, technology start-ups and legislation. Our goal in dissemination is to ensure access and visibility of our findings and will prioritise high-quality open access peer-reviewed journals and interdisciplinary conferences. We will rely on the PDC to share key findings that can inform their goals and procedures to improve equity in the development of paediatric medical devices.
This review has been registered with the Open Science Framework (https://osf.io/k72bn) and protocol materials, amendments, and resulting data can be accessed there.
Discussion
The exploratory and foundational question we are seeking to address (‘What is known about the programmatic features that set up an institution to successfully support paediatric medical device research?) is ideally addressed by a scoping review methodology, which is intended to ‘… map the existing literature in a field of interest’ and is ‘… of particular use when the topic has not yet been extensively reviewed or is of a complex or heterogeneous nature’.34 By design, scoping reviews are heterogeneous and thus do not include structured quality assessments and other features of systematic reviews. Our scoping review will encounter limitations given the interdisciplinary nature of the topic, the elusive qualities of relevant grey literature and the language capacities of our research team. Several disciplines including medicine, engineering, public policy, law and economics play a contributing factor in the complexity of our topic. Each discipline has its own publication cycle and norms that need to be understood and incorporated to effectively retrieve the relevant literature. Grey literature is more difficult to seek out than published studies since it is traditionally not included in major academic bibliographic databases. While we have incorporated multiple strategies to capture relevant grey literature, we anticipate that we may still miss significant studies. There are several nuances to medical device regulation that may make abstract review challenging. For example, the differences between regulated SaMD and digital health applications continue to evolve, and abstract screening may not provide sufficient information. While we anticipate not finding articles that specifically discuss paediatric medical device research infrastructure in detail, there may be relevant insights in articles discussing specific trials. However, these insights, typically found in a discussion section, will likely not be apparent during abstract screening. Similarly, due to our focus on clinical trial infrastructure and papers involving human subject research, we might miss valuable insight included in the papers describing other medical device development stages. We acknowledge that the development of paediatric medical devices is a global issue and overcoming barriers is a global effort. However, we are limited to the language proficiencies of our team members and may be required to omit relevant studies based on language of publication.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank all of the staff, collaborators and colleagues at the five Pediatric Device Consortia and the FDA’s Office of Orphan Product and Development for their tireless support of paediatric healthcare innovation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @juanespinozamd
Contributors JE conceptualised the study and is the guarantor of the review. GZ, JE and LK helped design and lead the team in drafting the scoping review protocol. LK developed the search strategy, conducted preliminary literature reviews, set up Covidence and registered the review in Open Science Framework. CJK, FJ, JE, LK and UT conducted pilot title/abstract screening and finalised the inclusion criteria. ATS, FJ, GZ, HK, JE, LK, LM, MC, PS, JF, KT and KE contributed to the title/abstract screening process. ATS, JE and LK prepared the manuscript. GZ, JE and LK revised the manuscript based on reviewers’ feedback. LK, GZ, LM, MC, PS, FJ, HK, ATS, JF, UT, KT, CJK, KE and JE reviewed the manuscript and approved the final version.
Funding This work was supported by the Food and Drug Administration under award number P50FD006425 for the West Coast Consortium for Technology & Innovation in Pediatrics (PI: Espinoza). The funding source had no involvement in the development of this manuscript or in the decision to submit the paper for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the FDA.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.